Case Presentation MEN2A
© 2022 Hazem Rayyan, Yousof Al Alawi, Atyya Alzahrani, Ismail Gurbal, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Multiple endocrine neoplasia type 2 (MEN2) is an autosomal dominant disorder that can be distinguished as three different syndromes: multiple endocrine neoplasia type 2A (MEN2A). MEN2B and familial medullary thyroid carcinoma (FMTC). This disorder is usually caused by the mutations of the rearranged during transfection protooncogene gene (RET) or the neurotrophic tyrosine kinase receptor type 1 gene (NTRK1).
Introduction
Mutations in the E7 proto-oncogene on chromosome 10 have been identified in MEN 2A MEN 20 and familiallar Mauid carunama The RET protein is a receptor tyrosine kinase MEN JA and familial medullary thyroid carcinoma mutations result in activation of certain intracellular pathways.
Background
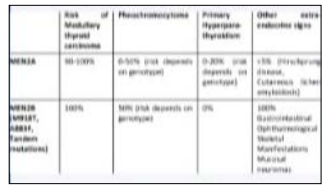
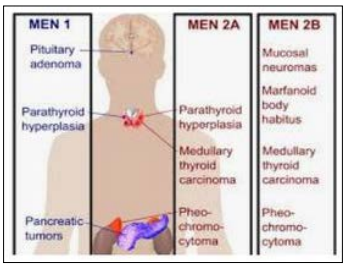
MEN2A is subdivided into four phenotypes:
- Classical MEN2AA family (or individual) with at least two MEN2A clinical features: MTC, PHEO, and/or HPT (includes: hyperparathyroidism, parathyroid adenoma, or parathyroid hyperplasia).
- MEN2A with CLAClassical MEN2A family (or individual) that also developed cutaneous lichen amyloidosis (CLA).
- MEN2A with HSCRClassical MEN2A family (or individual) that also developed Hirschsprung’s disease (HSCR).
- FMTCFMTC (familial MTC) is used when four or more family members had MTC only and no clinical evidence of PHEO, HPT, or any MEN28-specific non-endocrine clinical features in affected or at-risk family members. Note, FMTC may be a disease variant of classical MEN2A with decreased penetrance of PHEO and HPT.
Case report
34years old female patient refered from surgery clinic after thyroidectomy deo to thyroid nodules found to have medullary thyroid carcinoma, for follow up, during investigations found to have high calcitonin, pan CT for staging done, Showed bilateral adrenal adenomas. While bp is normal, and no palpitations,. 24 hour urine for catecholamins done, found to hve 3 tims upper normal. Physical examination was normal- no neoromas or other feturs After discussion with patient and her family dission made to do bilateral adrenalectomy.Patient started preparation with phenoxypensanmin, then after 2 weeks of medicine, she underwent surgery smoothly without complications. Hestopathology came with diagnosis bilateral pheochromocytoma, Hormonal replasment with thyroxine and steroids, fludrocortisone started.
Ret protooncogene requested for her came positive, Then requested for her kids found 3 out 5 kids positive The dissision to do total thyroidectomy for those who had positive ret mutation [1-4].
Images

Recommendations
- Identify the germline RET mutations in the etiology of multiple endocrine neoplasia type 2
- Explain the epidemiology of multiple endocrine neoplasia type 2.
- Review the use of total prophylactic thyroidectomy and lymph node dissection in the management of multiple endocrine neoplasia type 2.
- Summarize the importance of collaboration and communication among the interprofessional team to provide counseling and genetic testing to first degree relatives of those affected with multiple endocrine neoplasia type.
References
- Accardo G, Canzo G, Esposito D, Gambardela C, Mazzela M, et al. (2017) Pasquali D Genetics of medulary thyroid cancer. An overview. Int J Surg 1: 2-8.
- Brandi ML, Gagel RF, Angel A, Bischian JP, Beck Pecco P, et al. (2001) Tomasses Tonel Wels SA ir Manx SJ Gusteines for dagnosis and therapy of MEN type 1 and type 2 J Cin Endocrinol Metal 12: 568-571.
- Quayle FJ, Molay JF (2000) Medulary thyroid carcinoma: Including MEN 2A and MEN 28 syndromes J Surg Oncol 89:122-129.
- Wells GA, Drate H (2015) Revised American Thyroid Association guidelines for the management of medulary thyroid carcinoma,Thyroid.