Laparoscopy Supports Implementation of Primary Infertility Diagnosis and Treatment: Case Reports
© 2024 Deddy S Razak, Eddy Hartono, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Infertility is defined as conception failure in couples who have had sexual activity without regular contraception for one year and are still not pregnant. Abnormalities in the fallopian tube have the highest percentage of 30-45% as a cause of infertility. Hydrosalping is a condition where one or both fallopian tubes have fluid-containing clots and is the cause of 25–30% of all infertility cases. The condition of the fallopian tube and its patency can be detected with a hysterosalpingogram (HSG). Although a HSG examination can give a picture of the uterine cavity and tubes, other abnormalities such as adhesion and endometriosis are sometimes not detected. So, laparoscopy can be used to solve this problem.
Results: We reported that a 27-year-old woman, Para 0, Abortus 0, came to the gynecology department with a major complaint of infertility. At the HSG examination, an unpatented right fallopian tube was found. So, the patient underwent laparoscopy, but both fallopian tubes were found in a patent state, and there was a tubal attachment on the omentum and a paratuba cyst, so adhesionolysis and cystectomy were performed. It can be concluded that tubal abnormalities can be detected more clearly with laparoscopy than with HSG.
Conclusions: Laparoscopic is more recommended in cases of primary infertility, but further research to compare or combine these two modalities is still imperative.
Introduction
Infertility is defined as conception failure in couples who have had sexual activity without regular contraception for 1 year and still are not pregnant [1]. There are many factors that can cause infertility, such as abnormalities in the fallopian tube such as hydrosalping, anovulation, or adhesion conditions of the pelvic organs. Among the factors mentioned above, abnormality in the falopian tube has a 30-45% percentage as the cause of infertility [2,3].
Hydrosalping is a condition when one or both tubes are blocked due to the accumulation of fluid. Hydrosalping is the cause of 25–30% of all infertility cases in women, and the prevalence is around 30% in women with tubular abnormalities [4]. Most of them are asymptomatic, but hydrosalping can sometimes lead to abdominal or pelvic pain. Some women also experience abnormal bleeding symptoms. Diagnosis of this condition can be done by imaging the condition of the fallopian tubes that have undergone the examination of the hysterosalpingogram (HSG) [5].
HSG is a contrast fluoroscopic radiological examination performed to evaluate the uterine cavity, tubular tract, and peritoneum by using a contrast media injection through the cervical canal [6]. This examination can determine the pathogenicity of the fallopian tube, the contour of the womb, and the peritonium in the adjacent pelvic cavity in infertile patients. Sometimes, screening with HSG can find the aetiology that causes infertility conditions [7,8].
Although a HSG examination can provide information on the state of the uterine cavity and tubular patency, abnormalities such as adhesion and endometriosis are sometimes not detected [9-11]. Laparoscopy can provide a clearer picture of the condition of the fallopian tube or the adhesion of the peritoneum to the anatomy of the pelvic organs. Although HSG alone can determine the aetiology of the cause of infertility, it is not recommended as a first-line clinical evaluation test as it is an invasive procedure that also requires anaesthetic modality, thereby adding cost and side effects to the patient [12-14].
We have a case of a 27-year-old woman, Par 0, Abortus 0, who was hospitalised with infertility complaints for about 3 years after marriage with a history of HSG examination with a patented fallopian tube image and planned to undergo hysterolaparoscopy for further examination and follow-up on this patient.
Case Report
Ms. F. A 27-year-old Indonesian woman, Para 0, Abortus 0, came to the gynaecology department with a primary complaint that she had not had an offspring for about 3 years after marriage and was planned for hysterolaparoscopy. Patients have regular sexual intercourse two to four times a week. Other symptoms, such as waist pain, fever, and chamber disorder, are absent. History of menarche since the age of 11 Regular menstruation with a cycle of 28 to 29 days. There is no other history of illness. Vital signs are within normal limits.
The patient has a history of the first HSG examination (15/2/2022) of normal bilateral fallopian tube patents (Figure 1). Whereas from the ultrasound examination (16/8/2022), a hydrosalping picture is seen (Figure 2). whereas in the second HSG (27/12/2022), The right fallopian tube is enlarged, the walls are smooth, and there is no filling or additional defect or spill (-), which gives the effect of hydrosalping and non-patent right tubes. (Figure 3). Laboratory examinations and thorax photos were found within normal limits.
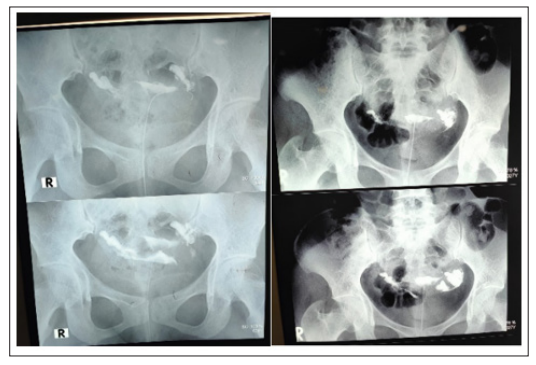
Figure 1: Results of the First HSG Examination
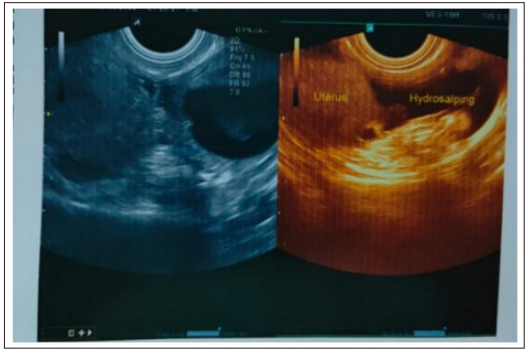
Figure 2: Ultrasound Results

Figure 3: Results of Second HSG Examination
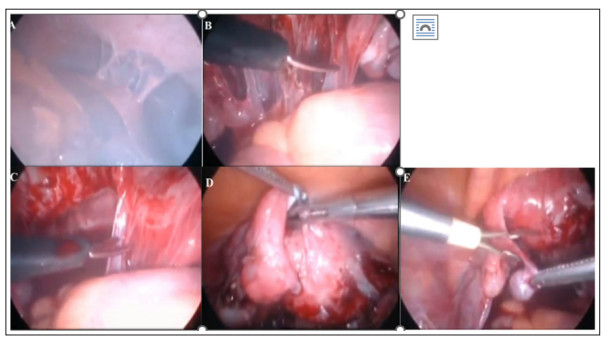
Figure 4: Diagnostic Laparoscopy and Adhesion (A) Fitz Hugh Curtis Sign Positive (B) Adhesion Picture Clearer (C) Adhesiolosis (D) Attention to the Left Falopic Tube Positive
Discussion
Infertility can be caused by many factors, such as abnormalities in the fallopian tube such as hydrosalping, anovulation, or conditions of adhesion of the pelvic organs. Among the factors mentioned above, anomalies in the falopian tube have a 30-45% percentage as the cause of infertility [2,3]. Hydrosalping is a liquid occlusion in the fallopian tube. Hydrosalping can be unilateral or bilateral, depending on the cause. Hydrosalping is associated with low rates of success in implantation and pregnancy. Some studies have shown that this condition affects the results of IVF, which is a decrease in the number of live births of about 50%. The hydrosalping fluid that has accumulated in the tube can flow into the cavity of the endometrium. This fluid can prevent embryonic implantation during the natural fertilisation process, even if one of the other tubes is patented and normal. This fluid is embryotoxic and can inhibit growth factors. In addition, hydrosalping fluids contain concentrations of protein and bicarbonate, contain inflammatory or infectious substances, lymphocytes, and other components, such as cytokines, prostaglandins, leukotrienes, and catecholamines, all of which can cause damage, infection, or immunological effects on the developing embryo and can make the endometrium unprepared for embryonic development. One study has investigated endometrial blood flow in patients with and without hydrosalping. The results of this study found that the endometrium of patients with hydrosalping experienced a significant decrease in blood flow compared to patients without hydroalping [15,16].
The exploration of the female genital anatomy is one of the vital elements in the assessment of infertility. Laparoscopy provides a comprehensive picture of the anatomy of the pelvic and abdominal organs [12,13]. It is generally accepted that diagnostic laparoscopy is the gold standard for diagnosing tubal pathologies and other causes of intraabdomenal infertility, such as pelvic adhesions [14,17,18]. However, this examination requires hospitalisation and anesthetics. HSG is the most commonly used diagnostic method for assessing tubular status and detecting intrauterine anatomical abnormalities in patients with infertility. Hydrosalping diagnosis can use both modalities. However, missed diagnosis often occurs from other ovarian abnormalities, such as tubo-ovarian abscess and cystic mass [19]. HSG does have a relatively low cost of examination and can be done as the first diagnostic procedure for assessing infertility. However, her diagnostic level is still underestimated. So, there are many other diagnostic strategies that can be used to overcome these HSG limitations, including laparoscopic examinations [18].
The exploration of the female genital anatomy is one of the vital elements in the assessment of infertility. Laparoscopy provides a comprehensive picture of the anatomy of the pelvic and abdominal organs [12,13]. It is generally accepted that diagnostic laparoscopy is the gold standard for diagnosing tubal pathologies and other causes of intraabdomenal infertility, such as pelvic adhesions [14,17,18]. However, this examination requires hospitalisation and anesthetics. HSG is the most commonly used diagnostic method for assessing tubular status and detecting intrauterine anatomical abnormalities in patients with infertility. Hydrosalping diagnosis can use both modalities. However, missed diagnostics often occur from other ovarian abnormalities, such as tubo-ovarian abscesses and cystic masses [19]. HSG does have a relatively low cost of examination and can be done as the first diagnostic procedure for assessing infertility. However, her diagnostic level is still underestimated. So, there are many other diagnostic strategies that can be used to overcome these HSG limitations, including laparoscopic examinations [18].
This patient comes with infertility complaints and asymptomatic symptoms. This patient has already undergone a related organ imaging verification that indicates the presence of hydrosalping. Hydrosalping is a clinical diagnosis with a comprehensive multiple examination by eliminating comparative diagnoses in patients. As far as the clinical diagnosis is concerned, it is based on the history, medical history, and physical examination of the patient. The diagnosis is then verified by radiography or supported by surgical results. At the time of the laparoscopy procedure in this patient, there was an extension of the two fallopian tubes in the abdomen organ, like the omentum, so an adhesionolyse was performed. In addition, with Methylene Blue, the findings of laparoscopy also found the fallopian tube in a patented condition. After adhesiolysis, cystectomy, and tubular patency tests, patients were diagnosed with pelvic inflammatory disease and paratuba cysts. Patients were treated with oral Doxycycline 100 mg tablets every 12 hours for 14 days as a response to pelvic inflammatory disease.
Conclusion
In this case report, a 27-year-old woman with P0A0 came to the gynecological department with infertility complaints for about 3 years after marriage. Hydrosalping is classified as a chronic cystic condition in the fallopian tube that forms after obstruction of the distal area tube and becomes one of the causes of infertility. At the HSG examination, the patient’s right fallopian tube was found without a patent, so laparoscopy was performed as a further examination and follow-up. At the laparoscopy, the two patented fallopian tubes were found with tube adhesion to the abdomen organ, such as the omentum, and a paratuba cyst was found. Thus, laparoscopy is more recommended in cases of primary infertility, but further research to compare or combine these two modalities is still imperative.
References
- Stevenson EL, Hershberger PE, Bergh PA (2016) Evidence- Based Care for Couples with Journal of Obstetric, Gynecologic & Neonatal Nursing 45: 100-110.
- Lindsay TJ, Vitrikas KR (2015) Evaluation and treatment of infertility. American family physician 91: 308-314.
- Otta SP, Reddy RG, Sangvikar S, Tripathy R (2022) Ayurvedic management of female infertility due to tubal blockage. Journal of Complementary and Integrative Medicine 19: 155-160.
- Tsiami, Chaimani A, Mavridis D, Siskou M, Assimakopoulos E, et (2016) Surgical treatment for hydrosalpinx prior to in-vitro fertilization embryo transfer: network meta-analysis. Ultrasound in obstetrics & gynecology: the official journal of the International Society of Ultrasound in Obstetrics and Gynecology 48: 434-445.
- Radswiki T, Rasuli B, Ibrahim D (2024) Hydrosalpinx. Reference article, Radiopaedia.org https://radiopaedia.org/articles/hydrosalpinx?lang=us.
- Simpson WL, Beitia LG, Mester J (2006) Hysterosalpingography: a reemerging Radiographics 26: 419-431.
- Chen LS, Zheng QZ, Jing L, Zhi TW, Ye Q, et al. (2020) Hysterosalpingo-contrast-sonography magnetic resonance- hysterosalpingography for diagnosing fallopian tubal patency: A systematic review and meta-analysis. European Journal of Radiology 125.
- Roest I, Kimmy R, Nienke W, Kim D, Marlies B, et al. (2021) Safety of oil-based contrast medium for hysterosalpingography: a systematic review. Reproductive BioMedicine Online 42: 1119-1129.
- Roest I (2021) Safety of oil-based contrast medium for hysterosalpingography: a systematic review. Reproductive BioMedicine Online 42: 1119-1129.
- Kahyaoglu S, Omer Hamid Yumusak, Inci Kahyaoglu, Gokce Naz Kucukbas, Alev Esercan, et al. (2017) Evaluation of time lapse for establishing distal tubal occlusion diagnosis during hysterosalpingography procedure performed by using water soluble contrast Journal of the Chinese Medical Association 80: 313.
- Chen S, Du X, Chen Q, Chen S (2019) Combined Real-Time Three-Dimensional Hysterosalpingo-Contrast Sonography with B Mode Hysterosalpingo-Contrast Sonography in the Evaluation of Fallopian Tube Patency in Patients Undergoing Infertility Investigations. BioMed Research International 2019: e9408141.
- Lee FK, Lee WL, Wang PH (2017) Is hysterosalpingography a good tool to confirm the patency of tubes? Journal of the Chinese Medical Association 80: 275.
- Laguerre MD, Arkerson BJ, Robinson MA, Moawad NS (2022) Outcomes of laparoscopic management of chronic pelvic pain and endometriosis. Journal of Obstetrics and Gynaecology 42: 146-152.
- Lorincz J, Jakab A, Török, P (2017) Comparison of current methods of tubal patency assessment Orv Hetil 158: 324-330.
- Ersahin SE, Nd G (2020) Surgical Removal of Hydrosalpinx Improves Endometrium Receptivity by Decreasing Nuclear Factor-Kappa B Expression. Reproductive sciences (Thousand Oaks, Calif 27.
- Volodarsky-Perel WB (2019) Treatment of hydrosalpinx in relation to IVF outcome: a systematic review and meta- analysis. Reproductive biomedicine online 39.
- Tan J, Min Deng, Meng Xia, Muhua Lai, Wenwei Pan, et al. (2021) Comparison of Hysterosalpingography With Laparoscopy in the Diagnosis of Tubal Factor of Female Infertility. Frontiers in Medicine 8: 720401.
- Foroozanfard F, Sadat Z (2013) Diagnostic value of hysterosalpingography and laparoscopy for tubal patency in infertile women. Nurs Midwifery Stud 2: 188-192.
- Hilwah Nora (2022) Hidrosalping bilateral dan infertilitas: laporan Jurnal Kedokteran Syiah Kuala. Nora https:// jurnal.usk.ac.id/JKS/article/view/27301/0.