Recent Advances in Endodontics – A Perspective Review
© 2021 Mithra N Hegde and Sembaga Lakshmi T, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Contemporary endodontics has seen an unprecedented advance in technology and materials. This article aimed to review some of the challenges and advances in the following sections: (1) Magnification, (2) LASER, (3) NiTi files, (4) Irrigation activation systems, and (5) CAD CAM. Jointly, these advances are aimed at improving the state of the art and science of root canal treatment and restoring the tooth back to function in the oral cavity.
Recent Advances in Endodontics - A Perspective Review
As science is constantly evolving, there are many innovative
instruments and materials at the disposal of a dentist. Over the past
few decades development in endodontics and restorative dentistry
took a leap with the advent of mainly 5 things which almost altered
the way in which dentistry was practiced earlier. This includes
magnification devices like Microscope, Lasers in dentistry, NiTi
Files, various irrigation activation systems and Computer Aided
Designing and Computer Aided Milling otherwise commonly
known as CAD-CAM. The scope of the current review is to give
a perspective of a dentist who is new to these technologies.
Magnification
Magnification devices were mainly invented to bridge the gap
between the vision of the naked eye and a microscope and it
includes magnifying glasses, loupes, Dental Operating Microscope
(DOM) [1]. Endodontist work with minuscule of anatomy and the
use of magnification cannot be over emphasized when working
in such constricted areas [2]. It has been shown through many
studies with the aid of magnification variation in anatomy like
second Mesiobuccal canal (MB2) and Middle Mesial Canals are
found with ease [3]. Retrieval of separated instrument is much
more predictable with the regular use of DOM. Earlier it was not
attempted due to the fear of creating more iatrogenic errors like
ledging or perforating the root canal system [4]. DOM gives a
superior ergonomics for the dentist allowing them to work for
longer hours without any musculoskeletal issues. Magnification
can be varied in a DOM depending on the type of case to low
(3x-8x), medium (8x-16x) and high (16x-30x) [5]. Endodontic
microsurgeries can be performed with high precision and less
trauma to the adjacent anatomical structure which in turn will
improve the number of patients being referred to the clinic. The
only drawback of DOM is the initial investment and the learning
curve that follows for its use in everyday practice [6].
Lasers
Laser is an acronym for Light Amplification by the Stimulated
Emission of Radiationand its first use dates back to 1960 by
Miaman [7]. Lasers in dentistry can be broadly classified into
hard and soft tissue lasers. Hard tissue lasers can be used in soft
tissue also but has its limitation of being expensive and inflicting
potential thermal damage to the dental pulp [8]. Carbon dioxide
(CO2), Neodymium Yttrium Aluminum Garnet (Nd:YAG) and
Er:YAG fall under the category of hard tissue laser and diode
lasers are classified as soft tissue lasers. Clinically laser can be
used for wound healing with low level laser stimulation therapy,
aphthous ulcer, photoactivated dye disinfection, aesthetic gingival
contouring and crown lengthening, frenectomies, removal of
inflamed or hypertropic tissues [9]. Laser fluorescence is used for
detection of caries. Hard tissue laser can be employed for caries
removal and cavity disinfection. Use of lasers should be done with
necessary precautions such as protective eyewear for everyone in
the operating room and proper disinfection protocols in place [10].
Niti Files
Before the introduction of Nickel Titanium (NiTi) in endodonics
by Walia, simple endo files were made of carbon steel or a stainless
steel. Stainless steel instrument have inherent stiffness which
increases as the size of the instrument increases. This led to a
lot of transportation of the canal, zip perforations to occur [11].
NiTi instruments on the other hand have shape memory and super
elasticity which made them more flexible thereby respecting the
curved and complexing root canal anatomy. From 1990 to now
NiTi instruments have undergone revolutionary changes in terms
of their construction to their physical characteristics [13]. The
objective was to preserves as much dentin as possible after shaping
the canal and negotiated thin curved canals without the separation
of the instrument [12]. There are 5 generation of NiTi files system and latest being the use of single file system for shaping the canal.
They can either be rotary or reciprocating based on their motion.
Examples of single file system include XP endo shaper, Hyflex
EDM which has the perfect combination of flexibility and fracture
resistance. This makes it possible to reduce the number of files
being used during a root canal treatment there by increasing the
speed of completion. For a brief period the was us of self-adjusting
file in the market which used scraping motion for cleaning and
has a hollow body throughout the file. This however did not last
in the market since they had to be used with a separate set of
engine system [13-15].
Irrigation Activation Systems
As we have become aware that endodontic infection is not just
by planktonic bacteria but by the biofilms to which they are
associated, it is imperative to destroy the biofilm in the process
of chemomechanical preparation. The shaping part of the root
canal system is taken care by advanced file systems whereas
the disinfection is mainly attributed to the irrigant employed.
The efficacy of the irrigant can be improved with adjunctive
activation systems. Various studies have shown reduction in the
bacterial load after activating the irrigant with ultrasonics. Newer
activation devices like Endovac (Discus Dental, Culver City,
CA), Photo Activated Disinfection, Photon induced photoacoustic
streaming (PIPS), and SWEEPS have been introduced in the
market. Of which endovac is an apical negative pressure irrigation
system with 3 basic components: A Master Delivery Tip (MDT),
the Macrocannula and the Microcannula. During irrigation, the
MDT delivers irrigant into the pulp chamber and siphons off
the excess irrigant to prevent overflow. The cannula in the canal
simultaneously exerts negative pressure that pulls the irrigant from
its fresh supply in the chamber by MDT, down the canal to the tip
of the cannula and out through the suction hose. This ensures a
constant flow of fresh irrigant being delivered by negative pressure
to working length [16].
PIPS uses low energy (50mJ, 10-15Hz) short pulses of Er:YAG for 50 microseconds. They create profound shock waves than cavitation which is seen in ultrasonics. Studies have shown that 17% EDTA and PIPS for 40 seconds can remove smear layer completely in the apical third simultaneously maintaining hydroxyapatite and collagen structure in the middle third indicating no thermal damage brought. PIPS along with 6% NaOCl shows complete removal of biofilm. Regular utilization of these techniques can enhance the clinical outcome of a root canal treatment [17].
Cad-Cam
In dentistry the major development for CAD CAM took place in
1980. Dr. Duret was the first to work on developing this system
way back in 1971 which led to the development of sopra system
[18]. The second is Dr. Moermann, the developer of the CEREC®
system. He attempted to use new technology in a dental office
clinically at the chairside of patients. He directly measured the
prepared cavity with an intra-oral camera, which was followed
by the design and carving of an inlay from a ceramic block
using a compact machine set at chair-side. The emergence of
this system was really innovative because it allowed same-day
ceramic restorations. When this system was announced, it rapidly
spread the term CAD/CAM to the dental profession [19]. The third
was Dr Anderson the developer of procure system. This system
later developed as a processing center networked with satellite
digitizers around the world for the fabrication of all-ceramic
frameworks [20].
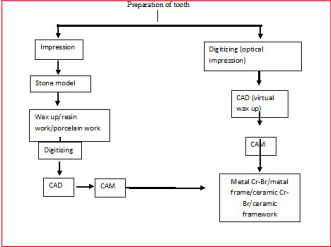
Workflow with a Cad Cam Set Up [21].
Conclusion
Gone are the days when endodontics was practice with just reamers
and patient being uncomfortable in a dental chair. The advent of
new technologies in dentistry has not only made the work flow
easy for the operator but also makes the dental treatment much
more comfortable for the patients. Endodontics in the present
era is practiced with much more predictable outcome than it was
done two or three decades ago. The future looks promising as
already researches are underway to clean the root canal system
without the need for shaping. It may take more time to come into
every day practice. What is already present must be utilized to
its fullest benefit.
References
1. Held SA, Kao YH, Wells DW (1996) Endoscope - An
endodontic application. J Endod 22: 327-329.
2. Brüllmann D, Schmidtmann I, Warzecha K, d’Hoedt B (2011)
Recognition of root canal orifices at a distance - A preliminary
study of teledentistry. J Telemed Telecare 17: 54-57.
3. Buhrley LJ, Barrows MJ, BeGole EA, Wenckus CS (2002)
Effect of magnification on locating the MB2 canal in maxillary
molars. J Endod 28: 324-327.
4. McGuigan MB, Louca C, Duncan HF (2013) Clinical
decision-making after endodontic instrument fracture. British
dental journal 214: 395-400.
5. Kim S, Kratchman S, Karabucak B, Kohli M, Setzer
F. (2017) Microsurgery in Endodontics. New Jersey:
John Wiley & Sons https://onlinelibrary.wiley.com/doi/
book/10.1002/9781119412502.
6. Kim S, Kratchman S (2006) Modern endodontic surgery
concepts and practice: A review. J Endod 32: 601-623.
7. Maiman TH (1960) Stimulated optical radiation in ruby lasers.
Nature 187: 493.
8. Parker S (2007) Laser regulation and safety in general dental
practice. Br Dent J 202: 523-532.
9. Marcusson A, Norevall L-I, Persson M (1997) White spot
reduction when using glass ionomer cement for bonding in
orthodontics: A longitudinal and comparative study. Eur J
Orthod 19: 233-242.
10. Armengol V, Jean A, Marion D (2000) Temperature rise
during Er: YAG and Nd: YAP laser ablation of dentine. J
Endod 26: 138-141.
11. Walia HM, Brantley WA, Gerstein H (1988) An initial
investigation of the bending and torsional properties of Nitinol
root canal files. J Endod 14: 346-351.
12. Moazzami F, Khojastepour L, Nabavizadeh M, Seied Habashi M (2016) Cone-beam computed tomography assessment of
root canal transportation by Neoniti and Reciproc single-file
systems. Iran Endod J 11: 96-100.
13. Gutmann JL, Gao Y (2012) Alteration in the inherent
metallic and surface properties of nickel-titanium root canal
instruments to enhance performance, durability and safety:
A focused review. Int Endod J 45: 113-128.
14. Metzger Z (2014) The Self-adjusting file (SAF) system: An
evidence-based update. J Conserv Dent 17: 401-419.
15. Thompson SA (2000) An overview of nickel-titanium alloys
used in dentistry. Int Endod J 33: 297-310.
16. Susila A, Minu J (2019) Activated Irrigation vs. Conventional
non-activated Irrigation in Endodontics-A Systematic Review.
Eur Endod J 25: 96-110.
17. Olivi G (2013) Laser use in endodontics: evolution from
direct laser irradiation to laser-activated irrigation. J Laser
Dent. 21: 58-71.
18. Duret F, Preston JD (1991) CAD/CAM imaging in dentistry.
Curr Opin Dent 1:150-154.
19. Mormann WH, Brandestini M, Lutz F, Barbakow F (1989)
Chair side computer-aided direct ceramic inlays. Quintessence
Int 20: 329-339.
20. Andersson M, Oden A (1993) A new all-ceramic crown: a
dense-sintered, high purity alumina coping with porcelain.
Acta Odontol Scand 51: 59-64.
21. Miyazaki T, Hotta Y, Kunii J, Kuriyama S, Tamaki Y (2009)
A review of dental CAD/CAM: current status and future
perspectives from 20 years of experience. Dental materials
journal 28: 44-56