Pre-Experimental Study to Assess the Impact of Awareness Program on Practice Regarding Bio-Medical Waste Management among Staff Nurses at Selected Hospital Kashmir
© 2022 Masood Ahmad Sheikh, Shabana Aazmeen, Uzma Paddar, Kirandeep Kaur, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
The aim of this study is to provide adequate awareness on practice among staff nurses regarding bio-medical waste management. Biomedical Wastes are those potential hazardous materials, consisting of solids, liquids, articles, sharps, and laboratory waste which pose a grave danger to the health of humans as well as other living organisms and in some cases, it may be lethal too. It is extremely important that the waste must be properly managed and disposed of safely so as to prevent outbreak of infections to general public and in health care settings in a society. According to the Ministry of Environment and Forests gross generation of biomedical waste in India is 4, 05,702 kg/day of which only 2, 91,983 kg/day is disposed, which means that almost 28% of the wastes is left untreated. The medical personals are more to get infection if not properly categorized and managed. Therefore, On the basis of these views a study was conducted to assess the impact of awareness program on practice regarding bio -medical waste management among staff nurses at selected hospital of Kashmir. For which 50 subjects were selected by purposive sampling technique. After data collection observational checklist was used to assess the practice among subjects. The data was analyzed by descriptive and inferential statistics by using chi-square and t-test. The findings revealed that the mean posttest practice level score (15.80), standard deviation 1.979, was significantly higher than mean pretest practice level score 13.96, standard deviation 3.319 among study subjects which indicated that observational checklist was highly effective in enhancing the practice among staff nurses at mean difference 1.84. The study also concluded that there were statistically no significant association between demographic variables (p=0.000) of staff nurses with their pre-test practice scores at 0.05 level of significance.
Introduction
The health care sector includes a diverse range of health care facilities, which have a size assortment from large general and specialist hospitals to small municipal dispensaries and D-type centers. All these facilities are an integral part of our society with an endeavor to reduce health problems and to eliminate imminent jeopardy to people’s health. In the course of curing health problems the health care sector produce a huge amount of bio-medical waste which may be hazardous to all those who come in contact with this waste. Hazardous waste management is a concern for every health care organization [1]. Biomedical waste (BMW) generated in our nation on a day to day basis is immense and contains infectious and hazardous materials. It is crucial on the part of the employees to know the hazards of the biomedical waste in the work environment and make its disposition effective and in a scientific manner. It is critical that the different professionals engaged in the healthcare sector have adequate Knowledge, Attitudes and Practices (KAP) with respect to biomedical waste management. Many studies across the country have shown that there are still deficiencies in the KAP of the employees in the organizations and hence it is necessary to make the appraisal of the same [2].
Biomedical waste poses various health and environmental hazards. Hence, it should be handled with the utmost care and disposed of safely. Several lacunas exist in the management of biomedical waste in India, and the pandemic posed by the coronavirus has made it even more challenging. The sudden outbreak of the virus led to an exponential rise in the quantity of biomedical waste. Furthermore, the poor infrastructure and lack of human resources have aggravated this situation. To combat this serious problem in a timely manner, the government has formulated various standard operating procedures and has amended the existing rules and guidelines [3].
Bio-medical waste’ (BMW) means any solid and/or liquid waste including its container and any intermediate product, which is generated during the diagnosis, treatment or immunization of human beings or animals or in research pertaining thereto or in the production or testing thereof [4].
Many wastes are produced as a result of human activities. Such waste may be dangerous and therefore need safe disposal. Industrial waste, sewage and agricultural waste pollute water, soil and air and it can also be dangerous to human beings and environment. Solid waste can be classified into different types depending on their source which includes House hold waste, Industrial waste, biomedical waste, hospital waste and infectious waste. Hospital waste is considered as hazardous because they contain toxic substances. This waste is generated during the diagnosis, treatment or immunization of human beings or animals or in research activities in these fields. Liquid waste can be divided into two components (a) Liquid reagents/ chemicals discarded and (b) the cleaning and washing water channel ed into the drain [5, 6].
Dental practices generate large amounts of waste paper, plastic, latex, and glass, much of which is contaminated with body fluids. An increasing variety of items that have hitherto been reused are now designed to be disposable, such as custom tips and triple syringe tips. Operating gloves are worn for almost all patient contact, resulting in a substantial increase in the amounts of latex and vinyl entering the waste stream. Surgical instruments such as local anesthetic needles, scalpel blades, and suture needles constitute a special category of contaminated sharp items. Dental practices also produce small amounts of waste mercury, silver and various solvents, and other chemicals [7].
Health care waste is a unique category of waste by the quality of its composition, source of generation, its hazardous nature and the need for appropriate protection during handling, treatment and disposal. Mismanagement of the waste affects not only the generators, operators but also the common people too [8].
India approximately generates 2 kg/bed/ day 3 and this biomedical waste encompasses wastes like anatomical waste, cytotoxic wastes, sharps, which when inadequately segregated could cause different kinds of deadly infectious diseases like Human immunodeficiency virus(HIV) hepatitis C and B infections, etc, and also cause disruptions in the environment, and adverse impact on ecological balance [9-12].
Hospitals are those institutions which have existed since time immemorial in one form or the other and have become more complex in the present time frequented by people from every walk of life without any distinction between sex, age, caste and religion. Recently, there is a significant increase in the dental and medical teaching hospitals and correspondingly there has been tremendous increase in the amount of biomedical waste generated by the hospitals. Biomedical waste [BMW] can be defined as “any solid, fluid or liquid waste, including its container and any intermediate product, which is generated during its diagnosis, treatment or immunization of human beings or animals, in research pertaining thereto, or in the, production or testing of biological and the animal wastes from slaughter houses or any other like establishments [13, 14].
Improper management of waste generated in health care facilities causes a direct health hazards on the society, the health care workers and on the environment. There is a requirement for the management of biomedical waste to minimize the risk of infection outside the hospital for waste handlers, scavengers and those living in the vicinity of hospitals. Management is also needed due to the risk of air, water, and soil pollution, or due to improper incineration emissions and ash. It plays an important role in disposal of the discarded drugs that can be repacked and sold off [15].
Keeping in view the above findings and from researchers own clinical experience the researcher realized that many of staff nurses are not aware regarding the bio medical waste management.. Lack of awareness about health hazards related to bio medical waste, inadequate training of proper waste management, practices, absence of waste management and disposal system, insufficient financial and human resources and low priority given to the topic are most common problems connected with the bio medical waste. Staff Nurses play a major role in the whole process. They need to be informed about current amendments in biomedical waste management rules and current technology to deal with biomedical waste. Therefore Sound knowledge and safe practices among them are to be strengthened.
In view of the above studies and magnitude of the problem, the investigator felt the need to assess the level of practice of staff nurses and make them aware of the Bio-medical waste management and so this study was undertaken.
Objectives of Study
- To assess pre-interventional practice scores regarding Bio -medical waste management among Staff nurses.
- To assess post- interventional practice scores regarding Bio -medical waste management among Staff nurses.
- To compare pre and post interventional practice scores regarding Bio -medical waste management among Staff Nurses.
- To determine association of pretest practice scores with selected demographic variables Gender, professional Qualification, Years of experience of Staff nurses.
Materials and Methods
A pre-experimental one group pretest posttest research design was conducted to assess the impact of awareness program me on practice regarding Bio medical Waste Management among staff Nurses in selected Hospital of Kashmir. Fifty subjects were selected by Purposive sampling technique. The tool consisted of demographic variables and observational checklist. Prior to data collection informed consent was obtained from the participants. The data was collected for analysis by using descriptive and inferential statistics.
The data presented in table 1 and figure 1 depicted that most of study subjects 45 (90%) were females and 5 (10%) were males respectively.
The data presented in table 2 & figure 2 revealed that as per professional qualification of nurses 30% GNM , 24% had post basic Bsc nursing degree, and (46%) had Bsc nursing degree.
The data presented in table 3 and figure 3 represented that maximum number of the study subjects 20 (40%) were having experience of >5 years, 18 (36 %) having 5-10 years of experience while as 12(24%) were having <10 years’ experience respectively.
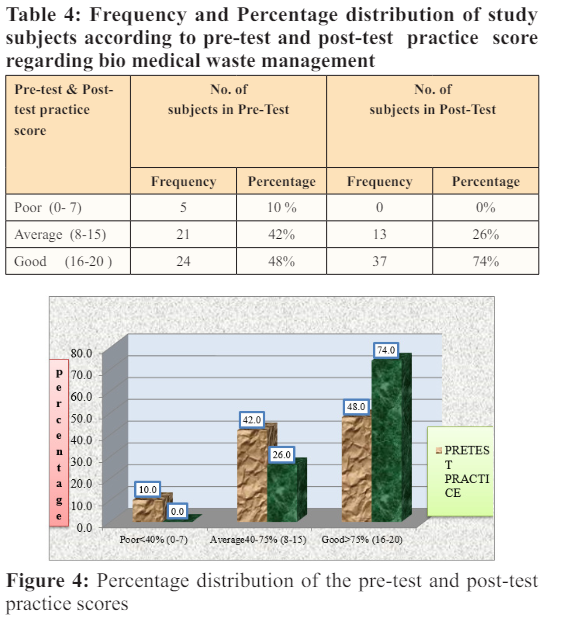
The data presented in table 4 and figure 4 depicted that in the pre-test 5(10%) of subjects had poor level of practice while as in the post-test none of the subjects had poor level of practice. Consequently, 21(42%) of subjects in the pre-test had ‘average level of practice’ and in the post-test only 13(26%) of subjects had average level of practice,. In the pre-test only 24(48%) subjects had good level of practice while as most of the subjects, 37(74%) had good level of practice in the post-test.
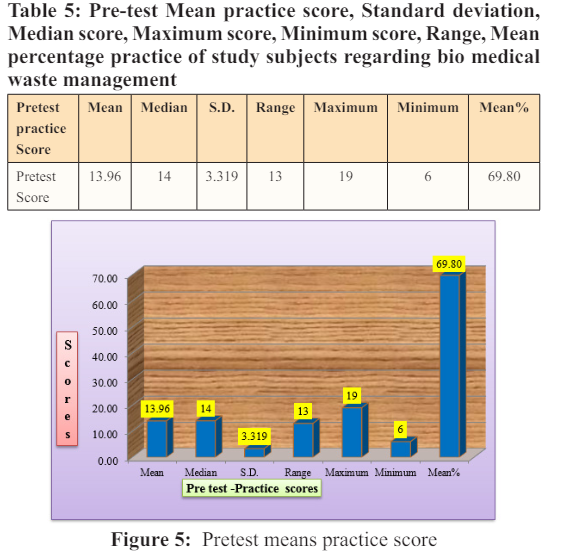
The data presented in table 5 & figure 5, revealed that the pretest (Mean ± SD) practice score of study subjects regarding bio medical waste management was (13 .96 ± 3. 319), Median was 14, Maximum score was 19, Minimum score was 6, Range was 13 and Mean percentage knowledge score was 69.80.
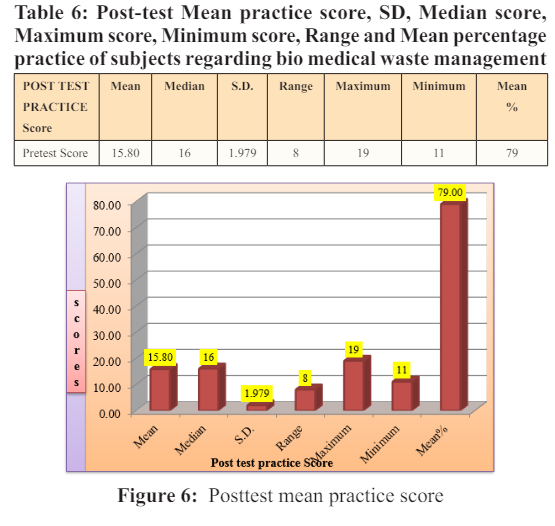
Table 6 & figure 6 showed that the post-test (Mean± SD) practice score was (15.80.± 1.979), Median score was 16 Maximum score was 19, Minimum score was 11, Range was 8 and Mean percentage practice was 79.00.
Recommendations
The Following studies can be undertaken in relation to present study:
- Similar study need to be undertaken with a large number of samples for better generalization.
- A similar study can be conducted by seeking other variables.
- The study can be conducted among other medical personals to assess the practice regarding biomedical waste management.
- True Experimental research approach can be used.
- The study can be conducted among non-nursing personnel to assess their practice regarding biomedical waste management.
- Setting can be changed by involving more hospitals and nursing homes.
Conclusion
The following conclusions were drawn on the basis of the findings of the study
- Pretest findings showed that the practice among staff nurses was found poor regarding biomedical waste management.
- There was improvement in practice of study subjects after the implementation of observational checklist regarding biomedical waste management practices.
- The observational checklist was found effective in improving the practice regarding bio medical waste management as it was evident from posttest knowledge score.
- The findings of study also concluded that there was no significant association between demographic variables (Gender, professional qualification and years of experience) of staff nurses with their pre-test practice as (p-value<0.001) This indicates that an effective program of observational checklist regarding biomedical waste must be imparted on regular basis to pre-clinical nursing students in order to increase the knowledge and practice regarding biomedical waste management because they are more prone to get infection as they are in close contact with the patients and there by so as to prevent the disease and reduce morbidity and mortality.
Aknowledgement
With profound gratitude I am deeply indebted to my Esteemed Teacher and Guide Professor (Dr.) Mehmooda Regu Principal College of Nursing IUST Awanipora, who helped me in stimulating, suggestions, knowledge, experience and encouragement and helped me in all the times of research period. In addition of this finally I am deeply and heartedly grateful to all my family members who morally supported through the construction of view successfully.
References
- Sharma S (2010) Awareness about bio-medical waste management among health care personnel of some important medical centers in Agra. Int J Environ Sci Dev 1: 251-255.
- Divya Rao, Dhakshaini MR, Ameet Kurthukoti, Vidya G Doddawad (2018) Biomedical Waste Management; a study on assessment of knowledge, attitude and practices among health care professionals in a tertiary care teaching hospital. Biomedical and pharmacological journal 11: 1737-1743.
- Tudor-TL, Noonan CL, Jenkin LE (2005) Medical care waste management: a case study from the National Health Service in Cornwall, United Kingdom. Waste management 25: 606-615.
- Sharma AK (1998) Biomedical Waste (Management and Handling) Rules. First edition. Bhopal. Suvidha Law House 12.
- Daljit Kapoor, Ashutosh Nirola , Vinod Kapoor, RamandeepSingh Gambhir (2021) Journal of Environmental Health Science and Engineering 19: 831-836.
- Irin Hossain, Ashekur Rahman Mullick, Shazly Bari, Mohammad Tahsin Islam, Dr Irin Hossain, et al. (2020) Pandemic COVID-19 and Biomedical Waste Handling: A Review Study. JMSCR 8: 497-502.
- Treasure ET, Treasure P (1997) An investigation of the disposal of hazardous wastes from New Zealand dental practices. Community Dent Oral Epidemiol 25: 328-331.
- Kumar PVAG, Kapate R (2012) Knowledge, Attitude, and Practices of Health Care Waste Management amongst Staff of Nursing Homes of Gulbarga City. Journal of Pharmaceutical and Biomedical Sciences 19: 1-3.
- Patil AD, Shekdar AV (2001) Health-care waste management in India. J Environ Manage 63: 211-220.
- Nath PA, Prashanthini V, Visvanathan C (2010) Healthcare waste management in Asia. Waste Management 30: 154-161.
- Lakshmikantha H (2006) Report on waste dump sites near Bangalore. Waste management 26: 640-650.
- Misra V, Pandey SD (2005) Hazardous waste, impact on health and environment for development of better waste management strategies in future in India. Environment International 31: 417-431.
- WHO G, Solid W (1980) World Health Organization Regional Office for Europe. Copenhagen: World Cat 1-31
- Jindal AK, Gupta A, Grewal VS, Mahen A (2013) Biomedical waste disposal: A systems analysis. MedJ Armed Forces India 69: 351-356.
- Aggarwal H, Kumar P (2015) Need for biomedical waste management. J Med Soc 29: 58-59.