Immunofluorometrical Exploring of FSH Levels in the Serum of Patients with Histologically Verified Large-cell Lung Carcinoma (LCLC)
© 2025 Ivan Milosevic, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
It is already known in the science that the cells of some types of LCLC can produce gonadotropins. By following the levels of FSH, in the serum of LCLC patients, we could make some statistical conclusions how significant these levels would be in eventual future early diagnostic procedures, besides already existing tumormarkers etc. This work would connect the Oncology, Endocrinology and Immunology fields containing very interesting immunofluorometrical procedures, hormonal theories and statistical estimates.
Introduction
Generally, the Lung Cancers are malignant tumors of epithelial tissue, fast propagating and giving the bad prognosis. Large- cell lung carcinoma (LCLC), in short, is a heterogeneous group of undifferentiated malignant neoplasms that lack the cytologic and architectural features of small cell carcinoma and glandular or squamous differentiation. LCLC is categorized as a type of NSCLC (non-small-cell lung carcinoma) that originates from epithelial cells of the lung. LCLC is histologically characterized by the presence of large, undifferentiated cells that lack distinctive features of either squamous cell carcinoma or adenocarcinoma (other types of cancers). Typically seen in LCLC tumor cells are abundant pale staining cytoplasm and prominent nucleoli.
The newest revisions of the (WHO) “Histological Typing of Lung Cancer schema” include several variants of LCLC, including:
- Large Cell Neuroendocrine Carcinoma
- Basaloid Carcinoma
- Lymphoepithelioma-like Carcinoma
- Clear Cell Carcinoma
- Large Cell Carcinoma with Rhabdoid phenotype.
Some of Above Presented Types Can Produce Gonadotropins Follicle-stimulating hormone (FSH) is a gonadotropin, a glycoprotein polypeptide hormone. FSH is synthesized and secreted by the gonadotropic cells of the anterior pituitary gland and regulates the development, growth, pubertal maturation, and reproductive processes of the body. FSH and luteinizing hormone (LH) work together in the reproductive system
Structure
FSH is a 35.5 kDa glycoprotein heterodimer, consisting of two polypeptide units, alpha and beta. Its structure is similar to those of luteinizing hormone (LH), thyroid-stimulating hormone (TSH), and human chorionic gonadotropin (hCG). The alpha subunits of the glycoproteins LH, FSH, TSH, and hCG are identical and consist of 96 amino acids, while the beta subunits vary. Both subunits are required for biological activity. FSH has a beta subunit of 111 amino acids (FSH β), which confers its specific biologic action, and is responsible for interaction with the follicle-stimulating hormone receptor. The sugar portion of the hormone is covalently bonded to asparagine, and is composed of N-acetylgalactosamine, mannose, N-acetylglucosamine, galactose, and sialic acid. On the basis of above presented, we can make the following connection: LCLC-FSH.
Matherials and Methods
Certain number of blood samples from LCLC should be collected by venipuncture and preserved in refrigerator in small test tubes under propperly conditions.
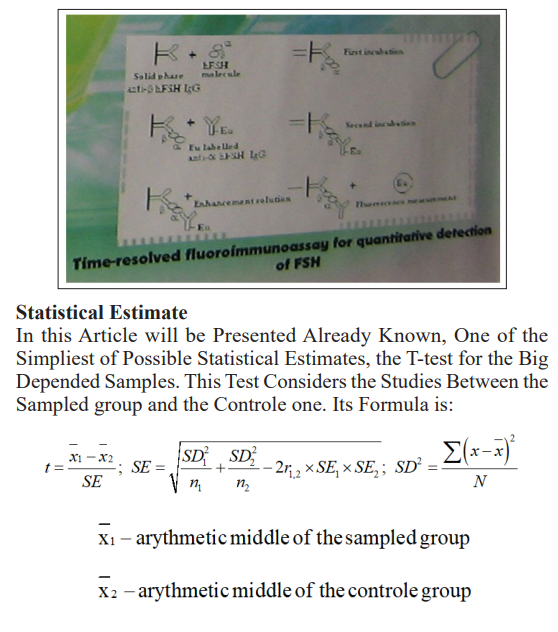
As an immunological part of this theoretical model, we will use time-resolved fluoroimmunoassay for quantitative detection of FSH.
In the first step we have solid phase anti(beta)hFSH IgG + hFSH molecule. After the first incubation, we get bonded hFSH to anti(beta)hFSH IgG by its (beta) part, where (alpha) part remains free. In the second step, we are adding Eu labelled anti(alpha)hFSH IgG, and, after second incubation we get enhacement solution, bonded two complexes. Eu that way remains free so that way we can do fluorescence measurment and quantitative detection of FSH.
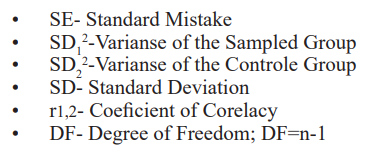
Discussion and Conclusion
On the base of following the levels of FSH in patients with verified LCLC as a target population, in so doing, following the levels of FSH in population with risk factors for LCLC, as a study population, in so doing, following the levels of FSH in randomly chosen population not belonging with two previous categories, as a control group. Comparation of these levels could lead us to eventual values of FSH in risk group, and could serve us as a potential screening method for LCLC.
By following of FSH levels in the serum of LCLC patients and making determinate statistical conclusions about its importance, that procedure could be eventually used as one of early or advanced diagnostic methods concerning mentioned disease. What would we get with that? The histological verification is very slow and painfull. At the same time the biopsy as a very invasive method would be avoided.
When the tumormarkers (CA-50, NSE etc.) are in the question as a diagnostic methods, in a combination with the FSH levels exploring, could be more reliable.
Even the syndromes and diseases that appear as a consequence of high levels of FSH, in a combination with classical clinical picture of lung cancer, could direct us to the LCLC type and in that case, the exploring of FSH levels in the serum of those patients would be necessary and useful too.
Of course, using this presented procedure we should pay attention on sex, growth, age, day period, cycle period, because of variability of FSH levels depended of those factors, as to make a difference between the morning and afternoon samples, etc.
Course, for now, all presented represents just thinking, mostly theoretical, that must be supported experimentally by larger and more detailed exploring through the cooperation among immunological and biochemical labs as well as clinical and scientific-research centers in tight connection with LCLC research. Actually, I this paper is here in order to attract attention of potential interested researchers in these fields to develope it [1-13].
Concerning all above presented, in future establishing of this procedure, we would get a rapid, comfortable, and safe diagnostic method.
References
- Abul K Abbas, Andrew H Lichtman (2023) Basic Immunology, Elsevier inc 201-207.
- Abul K Abbas, Andrew H Lichtman, Jordan S Pober (2000) Cellular and Molecular WB Saunders Company 406-411.
- Carr DT, Holoye PY, Hong WK (1994) Bronchogenic Carcinoma. Textbook of Respiratory Medicine Ed by JF. Murray and JA Nadel 1528-1596.
- Guyton AC (1996) Endocrine System Medical Physiology 824-922.
- Patic VJ (1995) Serological Reactions. Medical Virology 487-534.
- DELFIA Wallac Oy Turky The Original Brosure for Assay Procedure 1-14.
- Jeftovic IM (1999) Univariantic and Bivariantic Statistical Models. Medical Statistics 80-128.
- Fernandez FG, Battafarano RJ (2006) Large-cell neuroendocrine carcinoma of the lung. Cancer Control 13: 270-275.
- Cotran RS, Kumar V, Fausto N, Robbins SL, Abbas AK (2005) Robbins and Cotran pathologic basis of disease. St Louis Mo Elsevier Saunders 762.
- Siegel RL, Miller KD, Jemal A (2016) Cancer statistics, CA Cancer J Clin 66: 7-30.
- Kupeli M, Koseoglu RD (2018) Large Cell Carcinoma with Adenocarcinoma in Lung. J Coll Physicians Surg Pak 28: 240-242.
- Pierce JG, Parsons TF (1981) Glycoprotein hormones: structure and Annual Review of Biochemistry 50: 465-495.
- Boulpaep EL, Boron WF (2005) Medical physiology: a cellular and molecular approach. St Louis Mo Elsevier Saunders 1125.