Author(s): Asif Muhammad*, Zaw Myint and Wint Wint Nyunt
Globally Tuberculosis (TB) and RR/MDR TB are among predominant public health problems and major cause of morbidity and mortality specially across many Asian and African countries. High number of missing TB cases, early detection of TB and early Drug Susceptibility Testing (DST) based appropriate treatment initiation also remains a challenge in many low to high burden TB countries.
WHO in 2020 recommended rapid molecular test Xpert MTB/ RIF & Xpert MTB/RIF ultra to detect TB and RR TB instead of smear microscopy, culture and DST for children and adults [1]. By 2023 onward (National Tuberculosis Programs) NTPs globally are gradually shifting to Xpert MTB/RIF Ultra (hereafter called Xpert Ultra) as initial test for TB and RR TB diagnosis simultaneously among TB presumptive. Xpert Ultra is with improved sensitivity and reliability of detection of MTBC as diagnostic sensitivity has been improved by the addition of two multicopy genes (IS1081 and IS6110), and a novel“;trace call”; while the single copy rpoB gene is used solely to determine RIF resistance. Trace call result does not provide information about the Rifampicin resistance as the sequence coded by the rpoB gene is not detected. Interpretation and management of patients with Trace call results may be a challenge at clinical settings.
Xpert Ultra specifically designed to address the challenges of paucibacillary samples and improve sensitivity. It has a lower LOD than Xpert MTB/RIF i.e 16 colony forming units [cfu]/mL and 131 cfu/mL, respectively [2].Thus Xpert Ultra has a higher sensitivity than Xpert MTB/RIF for the detection of MTB in smear-negative, HIV-infected patients, children, and in testing extrapulmonary specimens, with at least as good accuracy for rifampicin resistance detection.
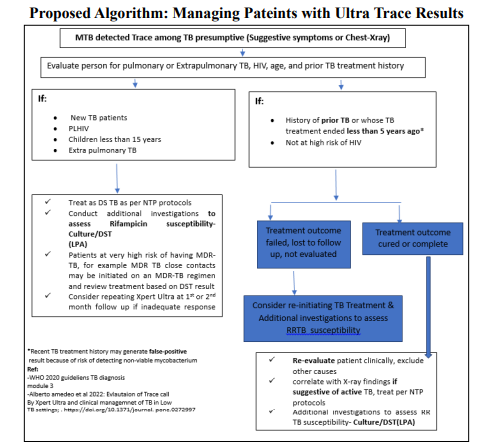
According to WHO, Ultra trace results are considered bacteriological confirmation of TB for: people living with HIV, children, individuals being evaluated for extrapulmonary TB, and adults being evaluated for pulmonary TB who are not at risk of HIV and who have not taken anti-TB treatment in the last 5 years. While for HIV negative (or not at risk of HIV) symptomatic adult patients with a recent history of treatment (i.e. completed < 5 years ago), Ultra trace results may be positive due to the presence of non-viable bacilli, rather than active TB. Therefore, treatment decisions must be based on the clinical and radiological judgment. However, WHO does not recommend repeating Ultra trace resuls [2].
The decision pathway to manage patients should include criteria for interpreting the“;MTB detected trace”; results, to balance the potential harms of overtreating patients with a false-positive result with the potential benefits of increased numbers of correctly diagnosed TB patients and decreased mortality associated with TB. It is to be noted that Xpert Ultra may give about 3 % of trace call results among all Xpert Ultra tested [3].But among ultra positive range of trace call could be 17-53% from low to high TB burden settings [4-5]. Trace call results may be more frequent if the sputum samples are suboptimal. Below is proposed algorithm for patient management pathways with Ultra Trace results.
A study conducted in South Africa defined predictors of active TB disease when faced with a positive trace result by Xpert Ultra and these are; EPTB samples, the presence of constitutional TB symptoms (more specifically in PTB patients) and no previous TB disease are independent predictors of active TB disease (TB culture positivity) in a high-burden TB setting. Moreover, the predictive ability was improved when TB symptoms were combined with TB CXR [3].
A study from Bangladesh where Trace call results have been repeated demonstrated that repeating Ultra- trace showed marginal improvement and acknowledged that such an approach of repeat testing may not be practical for implementation in a setting without extensive laboratory resources [4]. Moreover, still many clinicians may put patients on TB treatmnet having presumptive PTB with a TB-suggestive Chest -Xray despite result of Ultra-trace or Ultranegative even in the context of indeterminate rifampin resistance.
A study from Bangladesh where Trace call results have been repeated demonstrated that repeating Ultra- trace showed marginal improvement and acknowledged that such an approach of repeat testing may not be practical for implementation in a setting without extensive laboratory resources [4]. Moreover, still many clinicians may put patients on TB treatmnet having presumptive PTB with a TB-suggestive Chest -Xray despite result of Ultra-trace or Ultranegative even in the context of indeterminate rifampin resistance.
Conclusively, based on WHO recommendations and available evidence, it is suggested that Xpert Ultra Trace call results should not be repeated. Instead, clinical and radiological judgment should be exercised for treatment decision-making, especially for patients with a recent history of TB treatment. Moreover, it is important to remember that many patients may hide their previous TB treatment history, which may be categorized as new, necessitating clinical evaluation in the treatment decision pathway. Furthermore, Trace call results should be subject to culture and DST.
To overcome the gap in identifying missing TB cases, NTPs should reach the unreached population. They should widely adopt Chest X-ray in conjunction with Computer-Aided Detection/Artificial Intelligence (CAD/AI) and WHO-recommended rapid molecular tests for the screening and diagnosis of TB. This is aimed at phasing out smear microscopy for TB diagnosis.