Author(s): Wolf-D Beecken*, Benedikt Hoeh, Felix KH Chun, Giordano Blume and Max Kersting
Introduction: Erectile dysfunction affects up to 30% of men in industrialized nations. Although the disease is more common in older age, men in their 30s and 40s are also affected. Despite the quantity and the important socio-psycho-pathogenic significance of erectile dysfunction, it is still treated almost exclusively by the administration of phosphodiesterase 5 inhibitors.
Objective: To evaluate the effectiveness and acceptability of a digital lifestyle change intervention for men with erectile dysfunction. Material and Methods: In this pilot study, 20 patients with erectile dysfunction were encouraged to make lifestyle changes using a digital application. Results: We were able to show that the use of a digital application is very effective in supporting the lifestyle change efforts of patients with erectile dysfunction.
Conclusion: Digital applications could offer valuable assistance in extending the purely symptomatic therapeutic approach (PDE5I) of men suffering from erectile dysfunction, to include the important component of lifestyle change in order to address the long-term implications of this complex condition
Worldwide, approximately 320 million men will be affected by erectile dysfunction (ED) by 2025 [1]. A clinical picture that leads to psychological and social problems for the affected person and their environment and can be an early indicator of serious cardiovascular events [2, 3].
Despite these far-reaching consequences of ED, this clinical picture is not given the necessary attention in the world’s health care systems. For example, in the German national health care system, the disease is included in a corresponding catalog as a so-called lifestyle problem, and any treatment of ED may not be charged by physicians (if sanctioned) to the community health care system [4].
Furthermore, the ED is a complex clinical picture due to its large scope, which requires complex diagnostics and communication with the affected person. However, due to the aforementioned problems, little attention is paid to this diagnostic, communicative and psychological complexity. Since the end of the 1990s, phosphodiesterase 5 inhibitors (PDE5I) have been available as a therapeutic agent that is effective in many cases of ED. However, the diagnostic and psychological components of medical work are often completely neglected and a corresponding prescription is issued directly when the patient merely hints at such a problem [5]. However, the good efficacy of PDE5I in this context is purely symptomatic. The underlying problem, whether psychological or organic in nature, is not treated by the active substances [6]. Since an investigation into the cause of the individual’s ED prior to prescribing PDE5Is is often absent, or the drugs are obtained through unofficial sources, this can lead to a constant worsening of the underlying problem and associated life-threatening complications. Therefore, both the American and British guidelines for the diagnosis and treatment of ED call for mostly risk-adapted diagnosis before treatment [6, 7]. Furthermore, numerous treatment options for ED are known and established, and the guidelines call for an individualized treatment
concept, taking into account all available treatment options and the needs and wishes of the affected person or couple.
One of the most important tools in the long-term treatment of ED is lifestyle modification with increases in physical activity, weight loss, smoking cessation, alcohol reduction, pelvic floor exercises, and stress reduction [8]. However, it is consistently pointed out that this lifestyle modification alone is often not sufficient for satisfactory treatment of ED. This therapeutic concept must be combined with other therapeutic options, such as medication with PDE5I, the use of a vacuum pump, hormone therapies or other modalities to be able to achieve a satisfactory therapeutic effect.
The application of lifestyle modification in itself represents a complex therapeutic procedure, which is increased in complexity by the addition of further treatment modalities. Unfortunately, therapy compliance with such complex therapies is very poor and therefore the expected therapeutic effect is not good without appropriate guidance [9]. It is understandable that even specialized physicians are not able to monitor and guide such a complex therapy concept purely in terms of time. This is where digital applications (apps) come into play. The cell phone has become a constant companion in everyday life. It surrounds us all day and is usually checked by the user at least every hour [10]. This makes the cell phone, in combination with a special app, the ideal instrument for implementing and monitoring such complex therapeutic procedures. We have designed an app to digitally guide and monitor a lifestyle change program (Regimen TM ) for men with ED. This app provides the user with a lot of information on topics such as, the development of ED, effects of increasing physical activity, the negative effects of smoking and alcohol consumption, nutritional information and many other topics in understandable knowledge texts. Furthermore, video instructions for pelvic floor and cardio training are given and regular breathing exercises for stress reduction are shown. For therapy controlled, daily erection tracking and regularly recurring surveys of International Index of Erectile Function questionnaire (IIEF-5) results are offered. The results of the surveys are compared to the initial results at onboarding to the app. During onboarding, an extended medical history and risk survey is used to classify risk, particularly for the presence of cardiovascular findings, and users are recommended to consult a specialist if they demonstrate an elevated risk profile [11]. In the present pilot study, we investigated the practical use, effectiveness, and user satisfaction of the app in 20 men with ED.
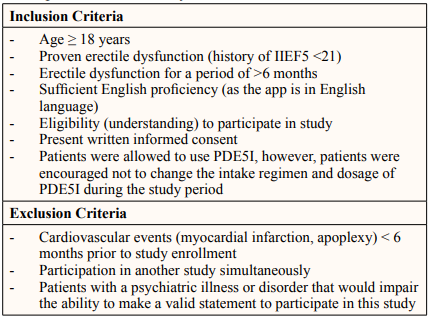
In a pilot study, the Regimen TM App was offered to twenty men with varying degrees of ED as the only or also as an additional therapy option. Written informed consent was obtained from all study participants, and the study was approved by the Ethical Committee at the Landesärztekammer Frankfurt (protocol 2020- 2007evBO). All study participants were recruited from the UroGate practice network in the Rhein-Main area (single center study) between 10/2021 and 06/2022. The inclusion and exclusion criteria can be found in Supplementary Table 1.
Supplementary Table 1: Inclusion and Exclusion Criteria to Participate within the Study
Patients were randomized to treatment (‘digital device’) or control group by simple 1:1 randomization. The treatment group received an activation code to access the app. The control group was given a concise information brochure which contained information about ED and what can be done to treat ED (exercise, diet, stop smoking, etc.). Subjects were assessed at study enrollment, 6 weeks and 12 weeks after enrollment (end of study).
Prior to treatment initiation, a general anamnesis as well as medical history questionnaire and the IIEF-5 were used to elaborate EDrelated history. The anamnesis questionnaire focused particular on the identification of causes of the ED, the period of existence of the ED and the identification of cardiovascular risk factors. At week 6 and 12, besides the IIEF-5 questionnaire, follow-up questionnaires elicited in particular the subjective satisfaction with the therapy instrument, the frequency of use, the influence on physical activity, diet, stress and the assessment of the usefulness of such a digital instrument for the treatment of ED and the health consciousness of men on the basis of rating scales from 0 (=no influence at all) to 10 (very positive influence). Furthermore, the frequency and type of side effects were ascertained.
Descriptive statistics included frequencies and proportions for categorical variables. Means and standard deviations (SD) were reported for continuously coded variables. The study population was stratified according to treatment and control group.
The chi-square test examined the statistical significance of the differences in proportions while the Kruskal-Wallis test was used to examine differences in means. Plots and pie charts were used to demonstrate outcome measurements over time according to each study assessment point.
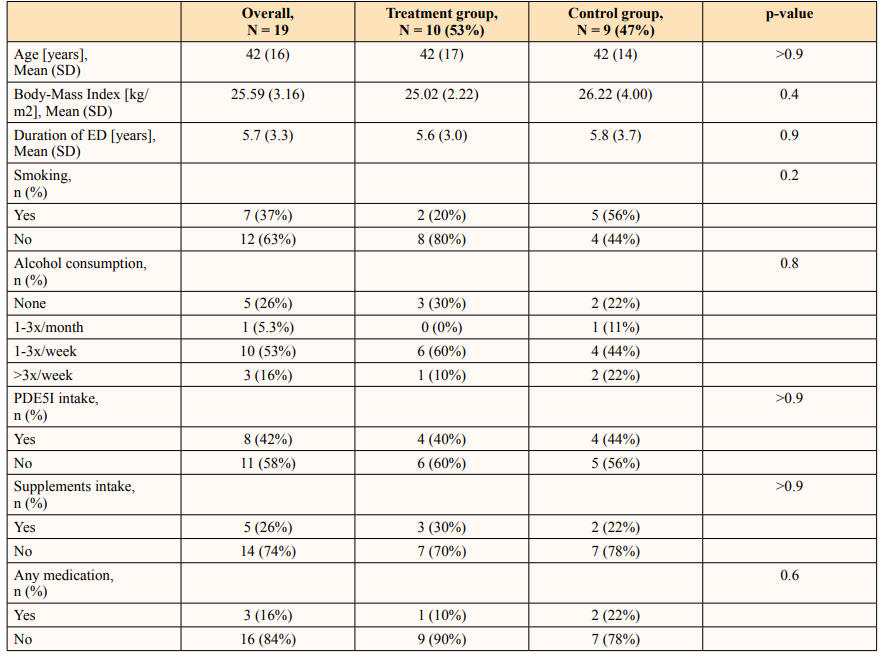
Of 20 patients, one patient (5%) was lost to follow-up prior to the first study visit and was excluded from all analyses whereas 19 (95%) patients completed the entire study protocol. Among those, 10 (53%) vs 9 (47%) were allocated to the treatment vs control group, respectively. Patient characteristics were comparable between the treatment and control group with a mean age of 42 (SD: 17) vs 42 (SD: 14) years and mean duration of ED of 5.6 (SD: 3) and 5.8 (SD: 3.7) years, respectively (Table 1). Rates ofPDEI-5 intake (40 vs 44%) and alcohol consumption (1-3xweek: 60 vs 44%) were comparable between treatment and control group (all p>0.05). Further patient characteristics can be found in Table 1.
At 12 weeks, 8 (80%) patients still reported using the app >3 times per week (at 6 weeks: 90%, Figure 1A) in the treatment group whereas in the control group 1 (11%) reported using the supplied information brochure (at 6 weeks: 0%; Figure 1B).
Figure 1: Pie Charts Depicting the Usage of the Digital Device in the Treatment Group (Figure 1a) and Usage of Information Brochure in the Control Group (Figure 1b) at Week 6 and Week 12

Regarding ED, mean IIEF-5 scores in treatment group increased from 10.4 (SD: 4.4) at study enrollment to 12.9 (SD: 5.5) at 6 weeks and 14.5 (SD: 4.9) at 12 weeks, yet without meeting statistical significance (p>0.05; Figure 2A). By contrast, IIEF-5 scores in the control group plateaued over time and ranged from 11.6 (SD: 5.8) to 12.1 (SD: 6.2) and 12.1 (IQR: 6.6) at study enrollment, week 6 and week 12 (p>0.05; Figure 2B).
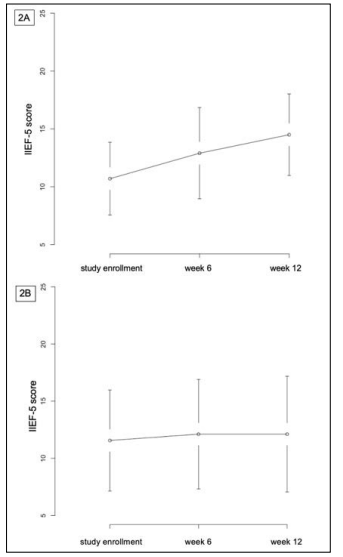
Figure 2: Graphs Demonstrating the Mean IIEF-5 Scores in the Treatment Group (Figure 1A) and Control Group (Figure 1B) at Study Enrollment, Week 6 and Week 1
High agreement values were shown in the treatment group compared to the control group, especially regarding interrogations on (a) &;ldquo;satisfaction with such a digital application for the treatment of erectile dysfunction” (At 12 weeks: 8 [SD: 1] vs 2 [SD: 3]; p<0.001) and (b) &;ldquo;influence of such a &;ldquo;digital” application for promoting men’s health awareness” (12 weeks: 9 [SD: 1] vs 3 [SD: 3]; p<0.001). It is of note that these findings were consistent and already prevalent at 6 weeks of study enrollment (Table 2).
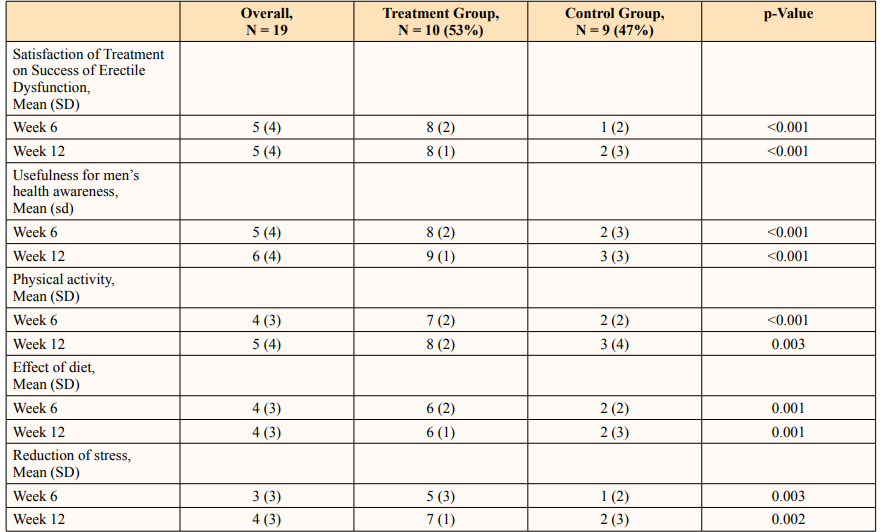
When examining the effects of treatment on physical activity (12 weeks: 8 [SD: 2] vs 3 [SD: 4]; p=0.003), diet (12 weeks: 6 [SD: 1] vs 2 [SD: 3]; p<0.01), and reduction of stress (12 weeks: 7 [SD: 1] vs 2 [SD: 3]; p=0.002), the treatment group showed agreement values in the middle range whereas the control group showed only low values (Table 2). Side effects did not occur in the control group, whereas two patients in the treatment group reported light joint problems.
ED and its frequent underlying causes (obesity, lack of physical activity, high stress levels, nicotine and alcohol abuse, etc.) represent a socioeconomic problem that has been neglected for many years. The psychological impact of ED and its associated impact on the work process has also been long recognized [2]. Despite the call in current guidelines for lifestyle changes to be taught as a fundamental treatment tool, the vast majority of cases are initiated on PDE5I purely as a symptomatic treatment [6]. This is conditionally understandable whether the complexity of a lifestyle intervention with known poor patient compliance [9]. On the other hand, it has long been known that especially in young men who develop ED, cardiovascular risk is significantly increased [12]. The coexistence of ED and the significantly increased risk for cardiovascular events (myocardial infarction and stroke) is probably to be found in the underlying lifestyle factors (especially lack of physical activity, obesity and stress) [12]. However, since the development of ED precedes such significant cardiovascular events by about three to five years in time, the therapeutic concept of lifestyle modification is of particular importance in two respects. On the one hand, the long-term curative therapy of ED, if possible, and on the other hand, early intervention to prevent the lifethreatening progression of cardiovascular disease patterns. In this respect, the complexity of the therapeutic concept of lifestyle modification and its poor compliance should not lead to a rejection of this important therapeutic option but should be an incentive for solving the problems associated with it.
The ubiquitous availability of the mobile phone, which nowadays closely accompanies the daily routine of most people, represents an opportunity to optimize such complex therapy methods. Already in 2016, data from more than 38,000 users of the Noom TM Coach smartphone app showed that such a digital tool is superior to the limitations of a paper-based diet plan in weight loss. This work also addressed the need to maintain treatment regimens [13]. We think that smartphone apps can provide a very unique opportunity in the institutionalization of complex therapy procedures. A successful complex intervention, such as a change in dietary behavior, or regular physical activity, each require habit change. Habits are powerful and changing them is extremely costly and difficult [14]. Once a new habit has been implemented, or an existing weak (compromising health) habit has been changed to a strong (promoting health) habit, this implementation/change is mostly sustainable. Regular smartphone use is an integral part of our habits. Additional adjustment of this habit to a complex therapy intervention is the task at hand.
In the present paper we describe, to our knowledge for the first time in the medical literature, the application of a digital instrumentto support the complex therapy procedure of a lifestyle change in men with ED. Although it is a very small observation group (n = 20), we were able to observe an improved therapeutic effect with regards to the IIEF-5 score (Figure 2A) within the treatment group. However, it should be noted that despite the observed tendency, it cannot be concluded that the patients experienced a clear clinically perceptible improvement in erection solely due to the digital app. Nevertheless, it should be noted that the mean IIEF-5 score of patients using the Regimen TM app was 10.4 at baseline and 14.5 after 12 weeks of app use, which improves moderate ED to mild to moderate ED.
Further landmark findings of this study, in our opinion, are particularly the satisfaction expressed by patients in the treatment group with a digital therapy approach in several respects: 1. Satisfaction with a digital tool for ED treatment (mean: 8 vs. 2 in treatment vs control group) on a 0-10 rating scale and &;ldquo;positive evaluation of a digital app for promoting men’s health awareness” (mean: 9 vs. 3 in treatment vs control group) on the aforementioned scale. These results are also confirmed by the fact that in the treatment group, nine out of ten subjects were still working with the app > 3x/week after twelve weeks. In our opinion, these results are all the more important because the effect on ED (IIEF-5 see above) was only slight.
In our opinion, the current results imply two necessities: 1. the long-term therapy approach, which we have already called for in our review from 2021, as well as 2. the necessity of a combination therapy with, for example, PDI5I [15]. Thereby, we assume that the primary good effect of PDI5I will lead to a significant treatment satisfaction and will further increase the compliance regarding lifestyle changes (this gives a good opportunity for habit change). Through this combined approach, the expected mediumto long-term effect of the lifestyle change can be manifested and, if appropriate, the medication can be reduced or discontinued in the further course. In addition, lifestyle modification, especially in younger patients (30 to 40 years of age), will have a positive effect on overall physical health and reduce high costs for the costintensive treatment of future cardiovascular events, if possible.
The occurrence of joint problems in two subjects from the treatment group, vs no side effects in the control group is probably due to the participants’ exercise. This result suggests that the subjects approached the treatment with much enthusiasm. Therefore, especially in overweight patients, the sports recommendations and instructions should be adapted to this risk.
The deficits of the present study are obvious. The group of subjects is by far too small to draw any further conclusions. The observation period should be extended significantly (> 1 year) in further studies. The combination therapy should be added as a further study group to verify our assumptions made here. Nevertheless, the results of this pilot study are quite encouraging regarding the treatment of patients with ED from purely symptomatic treatment to a possibly curative approach. Furthermore, these results should also be investigated in other conditions that may benefit from a complex extension of therapy, such as hypertension.
In the present study, it was shown that patients with erectile dysfunction benefit from a lifestyle modification. The support of the implementation of the modification with a digital app was judged to be extremely helpful. This study suggests that the complex therapeutic approach of lifestyle modification with the help of digital apps can experience a significantly higher compliance. Patients suffering from erectile dysfunction should definitely be offered digital support for lifestyle modification.
W.D.B., G.B. and M.K. are stockholders of the with o Inc, that is the producer of the Regimen App. The other authors declare that there is no conflict of interests.
All datasets generated for this study are included in the manuscript (supplementary files). W.D.B and B.H. had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
The study was approved by the Ethical Committee at the Landesärztekammer Frankfurt (Protocol 2020-2007evBO). All patients included in the study signed a written informed consent.
The research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Not applicable.