Author(s): Shahin Asadi
Majeed syndrome is characterized by recurrent episodes of fever and inflammation in the bones and skin. The two main features of this condition are chronic recurrent multifocal osteomyelitis (CRMO) and congenital dyserythropoietic anemia (CDA). CRMO causes recurrent episodes of pain and joint swelling which can lead to complications such as slow growth and the development of joint deformities called contractures. CDA involves a shortage of red blood cells which can lead to fatigue (tiredness), weakness, pale skin, and shortness of breath.Most people with Majeed syndrome also develop inflammatory disorders of the skin, most often a condition known as Sweet syndrome. Majeed syndrome results from mutations in the LPIN2 gene. This condition is inherited in an autosomal recessive pattern.
Majeed syndrome is a rare genetic disease that is repeatedly caused by fever and inflammation in the bones and skin. One of the major features of majeed syndrome e is inflammatory bone disease, known as chronic osteomyelitis (CRMO) [1].
Majeed syndrome can cause bone inflammation and relapse of joint pain and swelling in childhood or adulthood. These symptoms continue until adulthood, although they may improve for a short time. CRMO can lead to complications such as slow growth and the development of articular anomalies such as osteoporosis that limit certain mobility in the affected individual [1,2].
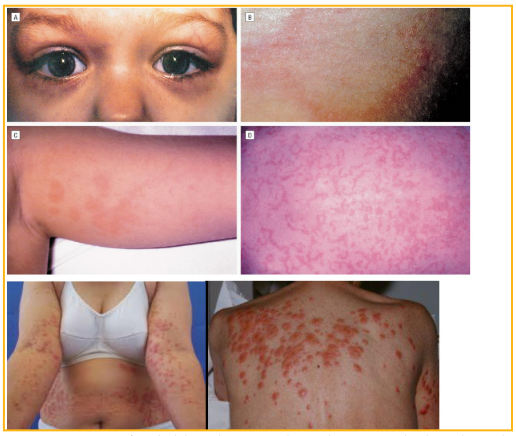
Figure 1: View of a child with Majeed syndrome with skin disorder
Another characteristic of majeed syndrome is blood and heart disorder, which is known as congenital anemia and congenital heart anomaly. This disorder is one of the different types of anemia, all of which include red blood cell deficiency. Insufficient red blood cells (erythrocytes), blood cannot transport enough oxygen to body tissues. Symptoms may include fatigue, weakness, tingling, and shortness of breath. Complications of congenital anemia and congenital heart disorder can vary from mild to severe. In addition, most people with majeed syndrome experience inflammatory skin disorders, also known as sweet syndrome. Symptoms of sweet syndrome include fever, nausea, vomiting, neck and back pain and skin tingling [1,3].

Figure 2: The picture of patients with sweet syndrome with inflammatory skin disorder.
Majeed syndrome is caused by a mutation in the LPIN2 gene. The LPIN2 gene is located on the short arm of chromosome 18 at 18p11.31. This gene provides instructions for the synthesis of a protein called leptin-2. Researchers believe that this protein may be involved in lipid metabolism. However, no lipid abnormalities have been identified with majeed syndrome. It is worth noting that leptin-2 protein may be involved in the control of inflammation and cell division. Thus mutation in the LPIN2 gene alters the structure and function of the leptin 2 protein. It is not yet clear exactly how these genetic changes in people with majeed syndrome lead to bone disease, anemia and skin inflammation[1,4].
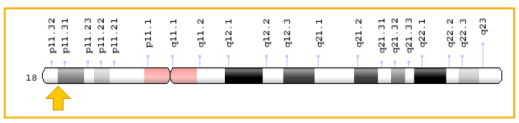
Figure 3: Schematic overview of chromosome 18 where the LPIN2 gene is located in the short arm of chromosome 18p11.31. Majeed syndrome follows an autosomal recessive inheritance pattern. Therefore, two copies of the mutated LPIN2 gene (one from the father and the other from the mother) are needed to cause the syndrome and the chance of having a child with Majeed syndrome is 25% for each possible pregnancy [1,5].
Majeed syndrome is a very rare genetic disorder that has so far been reported by only 3 families with this syndrome in the Middle East in medical literature[1,5].
Majeed syndrome is diagnosed on the basis of the clinical signs and symptoms of the patient using specialized pathological tests. The main method of diagnosis of Majeed syndrome is molecular genetic testing for the LPIN2 gene to investigate the presence of possible mutations. Prenatal diagnosis is also possible using amniocentesis fluid and sampling of fetal placental chorionic villi [1,6].
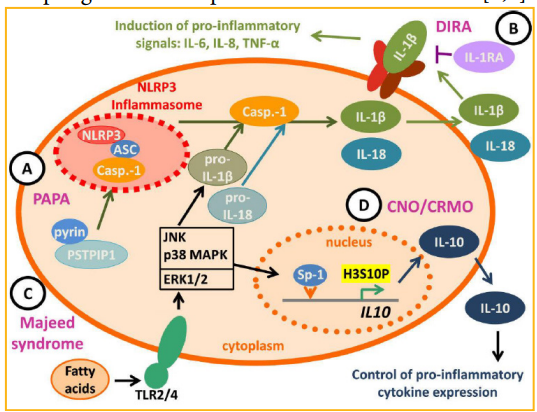
Figure 4: Schematic of the molecular genetic pathway of majeed syndrome. Treatment Options for Majeed Syndrome.
The treatment and management strategy for majeed syndrome is based on the symptoms and symptoms that are presenting to patients. Treatment may be done with the efforts of a team of specialists including a pediatrician, immunologist, orthopedist and orthopedic surgeon. Timely diagnosis and early treatment can be effective in improving the status of majeed syndrome patients. Genetic counseling is also needed for all parents who want a healthy child [1,7].
Majeed syndrome was first reported in November 1989 by Dr. Majeed HA [1,7].
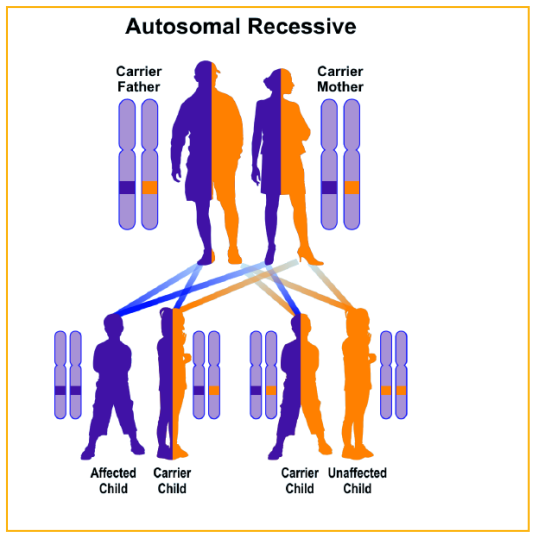
Figure 5: Schematic view of the autosomal recessive inheritance pattern, followed by majeed syndrome.
Majeed syndrome is an inherited skin disorder characterized by chronic recurrent multifocal osteomyelitis, congenital dyserythropoietic anemia and a neutrophilic dermatosis. It is classified as an autoinflammatory bone disorder. The condition is found in people with two defective copies (autosomal recessive inheritance) of the LPIN2 gene. LPIN2 encodes lipin-2 which is involved in lipid metabolism. The pathogenesis of this mutation with the clinical manifestations has not been elucidated. The prognosis has generally been poor because of progressive bone and hematological manifestations, however, outcomes have improved with more aggressive treatments. There is limited information on long-term outcomes in patients treated with IL-1 beta inhibitors but short-term follow-up has shown sustained clinical response to this biologic class [1,8].