Author(s): <p>Namratha Sai Reddy B, Nishith Vaddeboina* and Nirni SS</p>
Synchronous dual primary cancers have been reported in the past while majority of these are sporadic only few are hereditary. There have been a couple of case reports of synchronous primary ovarian cancer and renal cell carcinoma (RCC) and the first reported case was in 1988 by Myoga et al. Currently there is no clear explanation about synchronous RCC and ovarian cancers but steroid hormones & its receptors are thought to play a role. It is important for the clinician and the pathologist to rule out the possibility of metastatic deposits for the better management of the disease. Here we report a rare presentation of dual synchronous primaries of Clear cell RCC and High grade serous ovarian cancer in a 48year old female
Synchronous dual primary cancers have been reported with various histologies and various sites in the past. It is imperative for the clinician to differentiate primary from metastasis as the entire plan of treatment and prognosis changes. Warren and Gates in 1932 developed a criteria for making the diagnosis of coexistent primary tumors. This criteria included the following: (1) Histological confirmation of each of the tumors must represent a definite picture of malignancy; (2) There should be atleast 2cm of normal mucosa between the tumors and should be separated by at least 5 years (3) The probability of one tumor being a metastasis must be excluded [1]. With the increasing use of PET-CT imaging, there has been an increase in the trend of identifying suspicious lesion elsewhere in the body which is likely contributing to this increase in the incidence of dual primary malignancies.
In 2014, a regional cancer centre in India reported that among the 41 cases of multiple primary malignancies that were diagnosed between 2009-2012, 8 cases were synchronous (19.51%) and 33 cases were metachronous (80.49%). Head and neck cancers were the most frequent primary tumour sites, followed by gynaecological malignancies, breast cancer, lung cancer, esophageal cancer, and then the other types. The most frequent locations for the second type of cancer were the breast and gastrointestinal system, followed by lung and gynaecological cancers [2].
Here we report one such rare case of synchronous primary cancers arising from the kidney and ovary in a 48 year old female.
A 48-year-old G2P2 woman was incidentally detected with an abdominal mass when she visited a doctor for dyspepsia and bloating sensation of the abdomen. Routine ultrasound abdomen showed a solid cystic lesion in the right adnexa measuring around 5.5x6.0cm and a lesion in the right kidney measuring around 4x3 cm. The serum CA-125 level was 13.3 U/mL (normal, < 35 U/ mL). Computed tomography (CT) showed a right cystic adnexal mass measuring 8.5x7.0cm and another exophytic growth about 4.5x3.5 cm arising from the right kidney suggesting neoplastic lesion of right kidney and right Ovary. She had attained menarche & menopause at the age of 13 and 45 respectively, she had never undergone hormone replacement therapy and has no history of any malignancies in the family.
After a discussion at our institutional multi-disciplinary tumor board, this patient underwent right radical nephrectomy for right sided renal mass and total abdominal hysterectomy with bilateral salpingo-ophorectomy along with pelvic lymphnode dissection and omentectomy for the right sided adnexal mass. The postoperative histopathology report showed clear cell carcinoma with International Society of Urologic Pathologists (ISUP) Grade 2 with tumor limited to renal capsule with no lymphovascular and perineural invasion with all the 8 lymphnodes dissected being negative for malignancy and hence patient was staged as Stage 1 Right sided Clear cell renal cell carcinoma.
The postoperative histopathology report of the ovarian tumor showed high grade papillary serous cystadenocarcinoma with tumor size around 9x8x7cm ,confined to ovary and limited by capsule with no evidence of lymphnodal and omental metastases , so she was staged as stage IA high grade right sided carcinoma ovary.
Following discussion in the multidisciplinary tumor board meeting, considering the high grade of ovarian carcinoma, patient was advised 6 cycles of paclitaxel 175mg/m2 and carboplatin at AUC 5, once in every 3 weeks. This patient is due for 2nd of adjuvant chemotherapy next week.
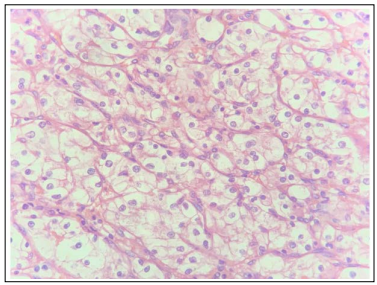
Figure 1: High power image of Clear cell RCC showing numerous single cells with well-defined cell membranes and round central nuclei with prominent nucleoli and pale cytoplasm
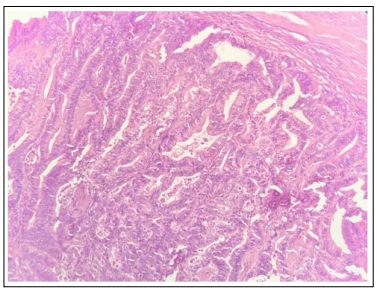
Figure 2: High power image of serous carcinoma of Ovary showing solid masses of columnar to cuboidal cells with eosinophilic cytoplasm and slit-like spaces with significant nuclear atypia and prominent nucleolus
Multiple synchronous primaries are rare and have been reported to be around 0.18% to 17% of cases in various retrospective studies [2,3].
Though the pathogenesis for these synchronous primaries have not been clearly described, according to one of the hypotheses, embryologically similar organs may produce synchronous tumours when they are exposed to hormones or carcinogens simultaneously [4]. Genetic susceptibility has been considered as one of the other hypotheses. This hypothesis suggests that with increasing availability of molecular testing methodologies like next generation sequencing, susceptible mutations have started to be studied. According to recent clinical research many genes, including BRCA2, ATM, POLD1, PALB2, SMAD4 and others have been linked to the development and pathogenesis of various primary cancers such as breast, ovarian, stomach, colorectum, uterine and pancreatic cancers [5-7].
It is quite uncommon for the kidney and the ovaries to present as synchronous primary neoplasms. There have been very few cases, in a case report by Balat et al, papillary serous ovarian carcinoma, which included both ovaries, a mixed (clear cell and granular cell type) renal cell carcinoma was also reported [8]. 3 cases of synchronous RCC and gynecological cancers were described by Wong et al., including one case of stage IV papillary serous ovarian adenocarcinoma [9]. Ringler et al. have reported a case of three simultaneous stage I primary tumours of the ovary, kidney, and lung [10].
This co-existence of RCC and organs like breast, ovary and uterus could be explained by the association of the steroid hormone target organs. The frequent correlation between steroid hormone organs and RCC may help to explain the association between RCC and organs such the breasts, uterus and ovaries. Di Silverio et al. reported 17 cases of RCCs with co-existent second primary neoplasms in tissues that are the targets of steroid hormones. 10 of these RCCs were linked to breast cancer, 4 to endometrial cancer and just 3 to ovarian cancer [11].
Except for the close association between the steroid hormone target organ ovary and RCC, this patient’s co-existence of synchronous RCC and ovarian cancer is not clearly linked by any identifiable characteristics. Even though RCC seldom metastasizes to the ovary or the other way around, histological confirmation of the underlying disease is still crucial for better management. The renal lesion was radiographically unclear and the right adnexal lesion exhibited a solid cystic lesion with internal septations, which are typical of malignancy. As radical or partial nephrectomy is the standard of treatment for small suspicious kidney masses, this patient underwent radical nephrectomy along with the debulking surgery at the same time, which helped us to confirm the diagnosis and stage the tumour appropriately. Considering the grade and histological subtype of the ovarian cancer, this patient was advised to receive adjuvant intravenous cytotoxic chemotherapy.
In addition to the diagnostic difficulty, the care for patients with multiple primary malignancies has substantial practical concerns like finding an appropriate therapeutic approach that addresses both cancer types while minimising side effects, relevant pharmacological interactions and adverse effects is a major problem. Even though it is exceedingly unlikely, clinical management should take into account the likelihood of coexisting RCC and ovarian cancer. Based on the pathologic and clinical features, special consideration should be given to the differential diagnosis between double primary and metastatic cancers.