Author(s): Anubha Bajaj
Severe mosquito bite allergy manifests as an uncommon cutaneous manifestation of natural killer (NK) cell subtype of chronic active Epstein Barr viral (CAEBV) infection. Predominantly documented in Japan, severe mosquito bite allergy characteristically delineates hypersensitivity to mosquito bites. Severe mosquito bite allergy is designated as an Epstein Barr virus (EBV+) induced NK cell lymphoproliferative disorder and represents as a cutaneous variant of chronic active Epstein Barr virus (CAEBV) infection.
Severe mosquito bite allergy manifests as an uncommon cutaneous manifestation of natural killer (NK) cell subtype of chronic active Epstein Barr viral (CAEBV) infection. Predominantly documented in Japan, severe mosquito bite allergy characteristically delineates hypersensitivity to mosquito bites. Severe mosquito bite allergy is designated as an Epstein Barr virus (EBV+) induced NK cell lymphoproliferative disorder and represents as a cutaneous variant of chronic active Epstein Barr virus (CAEBV) infection.
Severe mosquito bite allergy characteristically denominates an exaggerated allergic reaction to mosquito bites, incriminates diverse cutaneous surfaces and demonstrates a prolonged clinical course. Severe mosquito bite allergy is accompanied by complications such as hemophagocytic lymphohistiocytosis (HLH), hydroa vacciniforme-like lymphoproliferative disorder or systemic chronic active Epstein Barr virus (CAEBV) infection. Besides, enhanced possible emergence of overt NK/T cell lymphoma or aggressive NK cell leukaemia is encountered. The exceptionally discerned severe mosquito bite allergy predominantly incriminates Asians or Japanese.
Severe mosquito bite allergy preponderantly arises within children and young adolescents. Mean age of disease emergence is 6.7 years although the condition may appear between 0 to18 years. A specific gender predilection is absent [1,2]. Severe mosquito bite allergy is engendered due to hypersensitivity reaction following mosquito bites. Majority of incriminated subjects delineate elevated serum immunoglobulin E (IgE) along with enhanced Epstein Barr viral deoxyribonucleic acid (EBV DNA) load and circulating NK cell lymphocytosis confined to peripheral blood. Of obscure aetiology, severe mosquito bite allergy is associated with cogent genetic predisposition and environmental factors which influence disease pathogenesis [1,2].
Mosquito bite can induce expression of Epstein Barr virus latent membrane protein 1 (LMP1) within NK cells. Proliferation of mosquito antigen specific CD4+ T cells is associated with reactivation of latent Epstein Barr virus confined to NK cells. A proportion of infiltrating NK cells appear immune reactive to Epstein Barr virus (EBV).
Hypersensitivity to mosquito bite is engendered on account of proliferating CD4+ T lymphocytes arising as a reaction to secretions of mosquito salivary gland. Aforesaid secretions contribute to reactivation of Epstein Barr virus (EBV) within NK cells with the induction of latent membrane protein 1(LMP1). Constituent NK cells appear infected with monoclonal Epstein Barr virus (EBV) as delineated upon terminal repeat analysis. Besides, Epstein Barr virus terminal repeat analysis demonstrates monoclonal Epstein Barr virus in a majority of instances.
Akin to in situ hybridization (ISH) of hydroa vacciniformelike lymphoproliferative disorder, a fraction of NK cells exhibit Epstein Barr virus encoded small RNAs (EBERs) [3,4]. Simulating hydroa vacciniforme-like lymphoproliferative disorder, peripheral blood of severe mosquito bite allergy demonstrates latent membrane protein 1(LMP1), as discerned with polymerase chain reaction(PCR), thereby indicating the emergence of type 2 Epstein Barr viral latency [3,4].
Acute episodes frequently appear associated with pyrexia and general malaise. The condition exhibits acute, severe, localized cutaneous lesions manifesting as erythema, bullae, cutaneous ulcers or focal necrosis along with scarring. Besides, systemic symptoms as pyrexia, lymphadenopathy, liver abnormalities or hepatosplenomegaly may ensue. Lymphadenopathy and hepatosplenomegaly can be occasionally encountered [3,4].
The hypersensitivity reaction simulates hypersensitivity encountered upon injection site following vaccination. Upon resolution of hypersensitivity or symptomatic recovery, incriminated subjects appear asymptomatic until subsequent mosquito bite occurs. Severe mosquito bite allergy may progress to systemic chronic active Epstein Barr viral (CAEBV) infection with eventual emergence of aggressive NK cell leukaemia. Upon microscopy, cutaneous tissue obtained from incriminated site demonstrates epidermal necrosis, cutaneous ulceration and configuration of bullae. A dense infiltrate of lymphoid cells may extend into subjacent subcutaneous tissue [3,4].
Lymphoid infiltrate is polymorphous and comprised of miniature lymphocytes along with enlarged atypical cells admixed with diverse reactive inflammatory cells as histiocytes and eosinophils. Morphological countenance simulates hydroa vacciniforme-like lymphoproliferative disorder. Reactive CD4+ or CD8+ T lymphocytes appear intermingled within neoplastic lymphoid infiltrate [3,4].
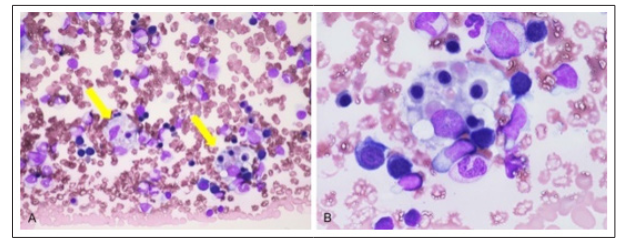
Figure 1: Severe mosquito bite allergy demonstrating EBV+ hemophagocytic T lymphocytes engulfing red blood cells and granulocytes [5].
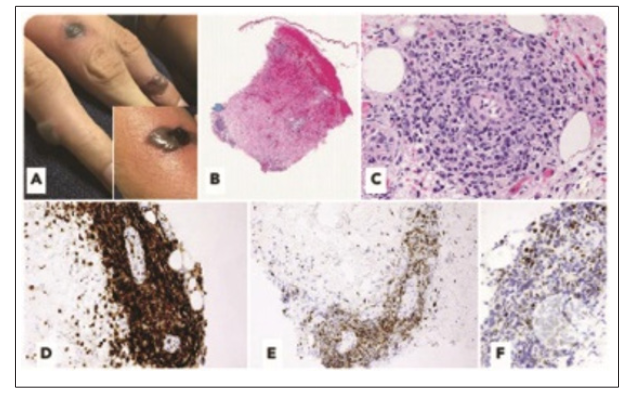
Figure 2: Severe mosquito bite allergy delineated erythema, bullae and cutaneous ulcers infiltrated by EBV+ T lymphoid cells admixed with enlarged atypical cells, reactive lymphoid cells as histiocytes and eosinophils confined to cutis with expansion into subcutaneous zones. Immune reactivity to diverse T cell markers is denominated [6].
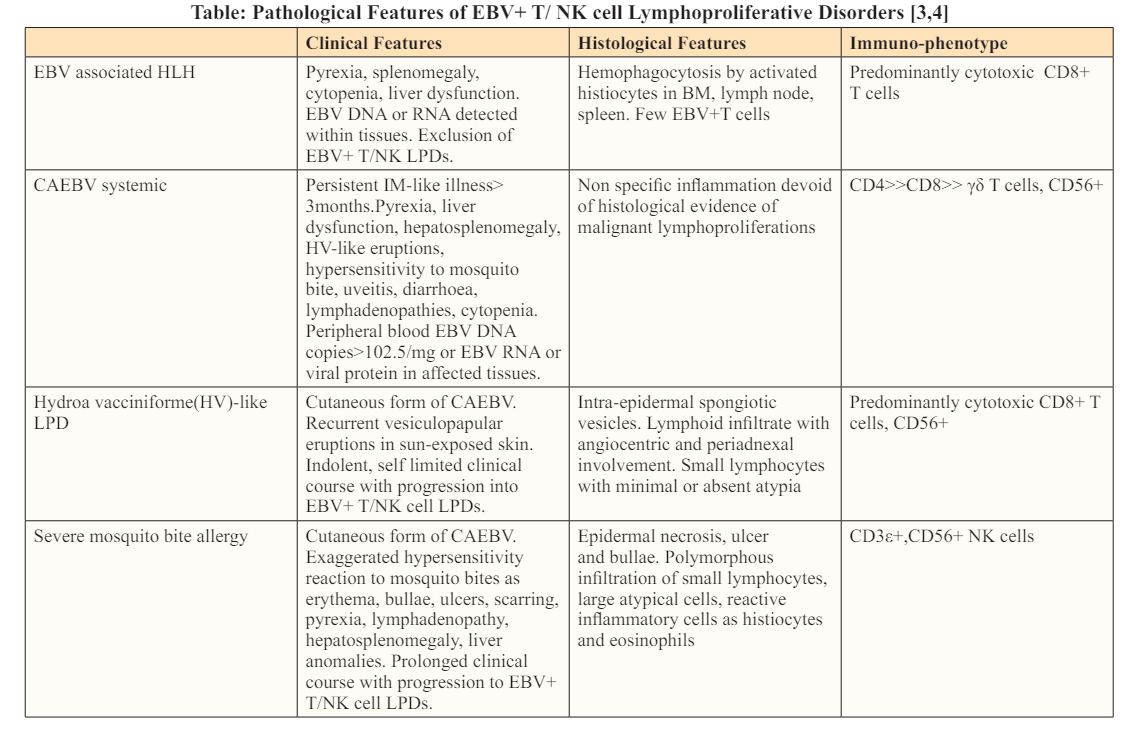
EBV: Epstein Barr virus, PTCL: Peripheral T cell lymphoma, HLH: Hemophagocytic lymphohistiocytosis, NK: Natural killer, BM: Bone marrow, CAEBV: Chronic active Epstein Barr virus infection, LN: Lymph nodes, TCR: T cell receptor, GIT: Gastrointestinal tract, LPD: Lymphoproliferative disorder, IM: Infectious mononucleosis
Although the morphological countenance is identical to hydroa vacciniforme-like lymphoproliferative disorder, infiltrating lymphoid cells exhibit an NK cell immuno-phenotype with expression of CD56 or cytotoxic granules T cell intracellular antigen1 (TIA1) and granzyme B. Epstein Barr virus infected neoplastic T lymphoid cells are frequently immune reactive to CD30+. However, cells are exceptionally immune reactive to latent membrane protein 1(LMP1)[7,8]. Neoplastic lymphoid cell infiltrate expands into subjacent subcutaneous tissue. Reactive CD4+ and C8+ T cells appear intermingled with infiltrating lymphoid cells. Infiltrating NK lymphoid cells appear immune reactive to CD3?+, CD56+ or cytotoxic molecules T cell intracellular antigen 1(TIA1) and granzyme B [7,8]. Thus, as latent membrane protein 1 (LMP1) is discerned within peripheral blood with polymerase chain reaction (PCR), severe mosquito bite allergy as a hypersensitivity reaction is contemplated to be an Epstein Barr virus latency type 2 disease [7,8].