Author(s): <p>Gideon K Kurigamba</p>
Juvenile polyps (JP) are rare but important causes of acute gastrointestinal symptoms in children. They are a recognized cause of painless rectal bleeding in preschool age children and also the most common intraluminal disorder of the colon in children
They are often solitary, pedunculated and small in size but may occasionally grow to large sizes or occur in great numbers, as in juvenile polyposis syndrome. Histologically juvenile polyps are similar to inflammatory polyps with irregular dilated glands, lamina propria expansion and granulation tissue expansion.
Sporadic juvenile polyps of the colon occur in up to 2 percent of children under the age of 10 years, are usually solitary, and are not associated with an increased cancer risk.
To share the experience of Juvenile polyposis, at Bwindi community hospital Uganda.
These are case reports of two children second degree relatives, who presented with recurrent rectal bleeding for 4 months after every passage of stool, with prolapse of a mass and were managed at Bwindi community hospital
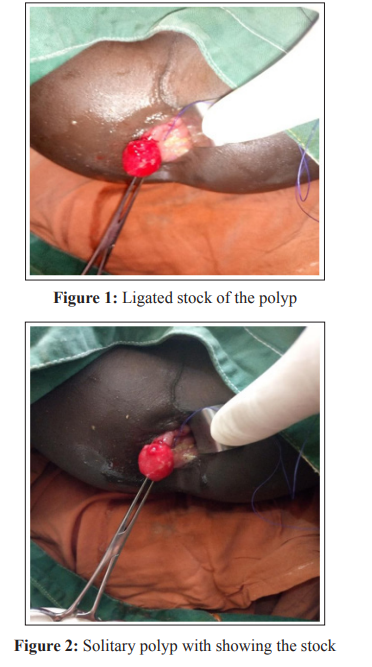
These patients were all admitted for a total of two days in Hospital. Average hemoglobin was 11.5mg/dl. Both had a pre-operative colonoscopy that revealed a solitary polyp in the rectal canal. They both underwent Examination under Anesthesia (EUA) and transanal polypectomy.
Juvenile polyps (JP) are rare, but a key cause of rectal bleeding in children and in low resource settings, transanal polypectomy remains the treatment of choice.
A 3-year-old girl was admitted to our surgical department with an on and off prolapsing anal mass for 4 months associated with rectal bleeding. There was no history of diarrhea, vomiting, constipation, abdominal distention, fevers or weight loss .Patient family history was negative for colorectal polyps or colorectal cancers.T. Current weight was 15kg and height of 34 inches
Abdominal examination was normal. Rectal exam revealed a pedunculated smooth round mass in the rectum at 12 O’clock with some visible fresh blood on the anal verge originating approximately 5cm from the anal verge.
Colonoscopy done revealed a 2-cm pedunculated polyp in the rectum while the rest of the large bowel and the terminal ileum were normal. Hemoglobin level was 12.1mg/dl, HIV test negative. Transanal polypectomy was done, the child recovered uneventfully and was discharged at day 1 post-operative with no recurrent episode of rectal bleeding at follow up. Histology of the resected polyp was compatible with juvenile polyp with no signs of dysplasia.
A 9-year-old boy presented to the surgical OPD with recurrent pinkish prolapsing anal mass on passage of stool since 2 years of age and occasional blood stained well-formed stools. He had no history of vomiting, constipation, abdominal distention, fevers or weight loss.
There was no history of a similar illness in the first degree relatives. However his cousin was recently treated at our facility with similar symptoms for an anal mass. Current weight was 24.8 kg, height -126 cm.
Rectal exam-solitary pedunculated smooth round mass in the rectum about 2 x 2 cm, CBC; WBC-6.53 x 109 (5-19 x 109 ) Haemoglobin-11.4 mg/dl (9.5- 14.1) MCV-81 fl (70-84), PLT326(150-450). Colonoscopy revealed a pedunculated polyp in the rectum, rest of the colon was normal. HIV test - negative
EUA plus trans anal polypectomy was done and the patient improved on postoperative analgesia and metronidazole, discharged on day 1 post-operative without any episode of bleeding. Histology of the polyp was compatible with juvenile polyp.
Juvenile polyp refers to the type of polyp (hamartomatous, usually limited to the colon), not the patient age [1].
Solitary juvenile polyps are among the most common causes of lower gastrointestinal bleeding in child hood.The rectal bleeding is recurrent in nature, like the case was with our second patient None of our patients had anemia or stunted growth which are some of the presenting symptoms in these children. Besides aneamia,infants can present with rectal prolapse too. Previous studies found rectal bleeding as the commonest symptom in (97.7%) and 78.5%. and the highest incidence of polyps was between ages 2 and 10 years 85.1%(6).Both of the patients were all under the age of 10 and rectal bleeding was one of the main symptom (100%) though non had any preoperative aneamia as evidenced by the CBC. Our two patients presented with per rectal bleeding and prolapse of a mass, but the pre-operative hemoglobin levels done showed no evidence of anemia [2-7].
Coburn et al 1995 found that 86.7% juvenile polyps located in the recto sigmoid area. Three percent of cases had a positive family history [ 7,8]. Our two cases all had rectal location of the polyps but with no previous noted family history.
Colonoscopy was done in these children and no other polyps were not seen. Colonoscopy is necessary in children since up to 60% of juvenile polyps are thought to occur in more proximal locations than the recto sigmoid junction and multiple polyps are associated with an increased risk of malignancy [4, 9].
Both of our patients under went examination under anesthesia and transanal polypectomy. A lone star retractor was necessary for the second older child.In a low resource setting like our study site trans anal polypectomy is a feasible and effective technique especially for polypectomy in low rectal polyps with minimal complications. This is a treatment of choice also when advanced endoscopic skills of polypectomy are not available.
Laparotomy to perform enterotomies and polypectomies may be needed. If there are clusters of polyps in isolated areas, limited segmental resection may be appropriate. Patients with numerous polyps in the colon may benefit from proctocolectomy with ileoanal anastomosis, which is required if adenomatous polyps with epithelial dysplasia are found [10].Solitary polyps should be removed by Colonoscopic polypectomies or transanal resection [4]. In our patients Trans anal resection was done.
Juvenile polyps (JP) are rare, but a key cause of rectal bleeding in children and a high index of suspicion is key in diagnosis.
Colonoscopic evaluation of children with rectal bleeding is essential in the diagnosis of juvenile polyps. Transanal excision of the polyps in low resource settings is sufficient for the polyps accessible through the anus.