Author(s): Camille B Toledo* and Dova M Sayon-Gonzalez
Objective: This study aimed to describe the sociodemographic and clinical profile of pediatric patients who consulted at the Out-Patient Department of a psychiatric facility in Davao City, ie. Southern Philippines Medical Center Institute of Psychiatry and Behavioral Medicine and provide baseline data for future research and program development.
Methodology: This is a descriptive chart review that used a purposive sampling method to determine the sociodemographic and clinical profile of patients below nineteen (19) years old, seen at the Out-Patient Department of a psychiatric facility from January 2015 to December 2019.
Results: A total of 427 charts were reviewed in this study. Majority (30.2%) of the study population had their first consult in 2019, female (56%), belonged to the 12-18 age group (64%), and had high school education (43%). Most came from Davao Region (89%) with class D social classification (64%). The clinical profile showed that majority consulted due to forensic reasons (54%), with referrals coming from WCPU, courts, or police stations (54%). Sexual abuse (43.9%) was the most common cause for forensic consult. The most common diagnosis was clustered under Adverse Childhood Experiences (30%). Most were advised referral to the psychology unit (59%) and were discharged as Out-patient (97%).
Conclusion: The number of child and adolescent consults in the Out-Patient Department of a psychiatric facility steadily increased within the span of five years. Majority of the patients came in for forensic reasons, with sexual abuse as the highest. A third of the consults were diagnosed to have Adverse Childhood Experience.
The World Health Organization (WHO) reported that disorders in mental health are one of the leading causes of diseases worldwide [1]. Studies have found that most mental disorders begin in childhood and adolescence where half of the mental illness commenced by fourteen (14) years of age [2-4]. Thus, understanding the degree, risk factors, and progression of such illness in this population should be highlighted [5].
Children’s mental disorders can be varied and present as grave changes in how children learn, behave, or regulate their affect that can cause distress in their daily activities [6]. Approximately 10-20% of children and adolescents have mental disorders, or an estimated 15 million, and can presently be diagnosed with a mental health disorder, including depression, anxiety, and conduct disorder [4,7]. A more significant number of children could be at risk of developing mental disorders due to factors in genetics, families, schools, and communities. Data showed an alarming number of children who have mental health problems had not received appropriate interventions compared to the 7% who do [8].
There has been little research on the mental health of children and adolescents in the Philippines compared to other developing countries [9]. WHO reported that 16% of children in the Philippines suffer from mental disorders [10]. The recent passage of the Republic Act 11036 or the Mental Health Act in the Philippines signaled that mental health is gaining importance among Filipinos. However, except for mental health promotions in schools, little was included for children and adolescents in this law which showed the need for additional development of child and adolescent mental health policy [11].
In many countries, including the Philippines, most of the funding for mental health services is dedicated to adult services. This made it difficult to the development of appropriate child and adolescent mental health services. Specific funding arrangements and policies should be facilitated for child and adolescent mental health services and should be regarded as separate health care [4]. The Out-Patient Department of the Southern Philippines Medical Center Institute of Psychiatry and Behavioral Medicine (SPMCIPBM) also caters to children who are brought in for a psychiatric consult. Still, this population is seen in the same setting as their adult counterparts which could hinder proper intervention for this vulnerable population.
Children are the nation’s most important asset, and proper promotion of their welfare should be implemented. The results of this study will serve as baseline data for the sociodemographic and clinical profiles of pediatric patients in the study area. This could be used in improving the services and establishing specialty training in the institution for enhanced service delivery specific to this population. This will benefit other researchers as a reference for further studies. Thus, this study aims to determine the sociodemographic (age, sex, address, social classification, educational attainment) and clinical profile (reasons for consult, diagnosis, outcome, referral to other services) of pediatric patients examined in the Out-Patient Department of SPMC-IPBM from 2015-2019.
This study utilized a descriptive retrospective chart review design. A purposive sampling method was conducted, wherein all charts of patients who were below 19 years old and who consulted at the Outpatient Department from 2015-2019 were included in the study. Only the initial consult was included for uniformity. The computed sample size at 95% confidence interval was 353.
The research protocol was presented to the department for approval and was then submitted to the Department of Health Cluster Ethics Review Committee (DOH-CERC). An expedited review of the protocol was done by DOH-CERC and was approved last August 10, 2021. Letters were then sent to the Department Chairman and Head of the Records Section to allow access to the charts for review. Data collection was then conducted. The charts were assigned a control number to ensure anonymity. To ensure privacy, the patients and their families were not contacted by any means (i.e. mail, electronic mail, phone, or social media) throughout the duration and even after the end of this study. A data-gathering form was utilized for the chart review.
The sociodemographic and clinical profiles of the study population were analyzed using descriptive statistics. Mean and standard deviation for continuous data such as the case of age and other relevant parameters measured using a standardized unit of measure. For categorical data such as the case of sex, type of management, and or procedure, frequency and the percentage were used to express the variables and data were summarized using frequency distribution table. Data analysis was encoded using Microsoft Excel software. Data analysis was done using Epi Info version 7. This software was favored over the other software because this is freeware and shareware software which is available at https:// www.cdc.gov/epiinfo/index.html.
A total of 427 charts were reviewed for this study, which was 20% more than the computed sample size of 353 at 95% confidence interval.
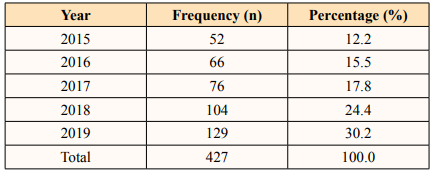
The majority of the study population had their first consult in 2018 and 2019 with 24.4% and 30.2% respectively (Table 1). The least number of child and adolescent patients were those seen in 2015 with a frequency of 12.2%.
The mean age of the samples was 12.6, where two (2) years old was the youngest and 18 years old was the oldest. The majority or 64.40% were teenagers or those in the 12-18 age group (Table 2). Those in their middle childhood or whose age ranges from 6-11 years old were 30.20% while those in the toddler and preschool years or those who were below 6 years old were only 5.40% of the population.
This study showed that a majority (56.4%) of the study population were female while 43.60% (186) were male. Eighty-nine percent (89.5%) of the study population were from Davao Region. Majority of the study population have attended school while 7% have not attended school. Forty-three percent (43%) of the study population have attended high school while 42% attended elementary school. Majority (64%) of the population were classified under the social class D while those belonging to social class C consisted of 36% of the study group.
The reason for consult was divided into forensic (53.9%) and non-forensic reasons (46.1%). It was noted that majority of patients who came in due to forensic or case filing were because of sexual abuse which was noted at 44%. This was followed by complaints of psychological abuse at 33%, physical abuse at 13% and evaluation of children in conflict of the law (CICL) at 7%. The top three non-forensic reason for consult include: behavioral and mood changes (8.70%), aggression (7.3%), and insomnia (5.60%).
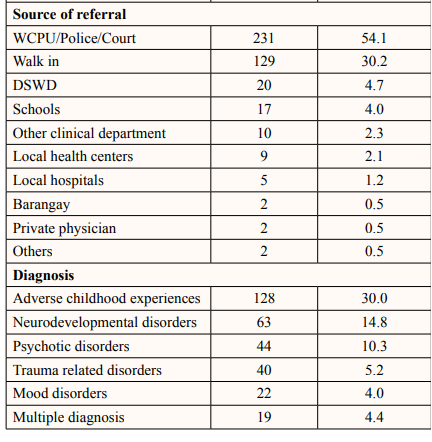
The study indicated that a majority (54.1%) of the study population were referred from the WCPU, police, or court. Other sources of referrals were walk-in patients (30%) and from centers run by the Department of Social Welfare and Development (DSWD) (4.7%).
Thirty percent (30%) of the population had a diagnosis of Adverse Childhood Experiences. Followed by Neurodevelopmental Disorders (14.8%) and Psychotic Disorders (10.3%).
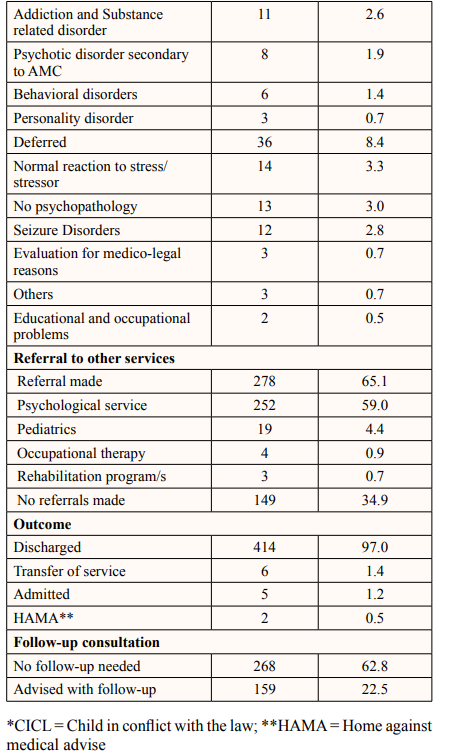
The study showed that most (65.1%) of the study population had been referred to other services (Table 3). Fifty-nine percent (59%) were referred to the psychological service for neuropsychological tests. Other referrals were made to the Department of Pediatrics (4%), Occupational Therapy (1%) and Rehabilitation programs for in and out-patients (1%).
It was noted that majority (97%) of the study population were discharged after their OPD consult. Those who were advised admission were 1.7% with 0.5% opted to go home against medical advice.
There was an increasing trend in the number of cases seen at the Outpatient Department from 2015 to 2019 (Table 1). The study supports the findings in a systematic review by Bor, et.al where various sources suggest an increasing burden of mental health problems in children and adolescents seen in the 20th and 21st Century [12]. Social changes such as worsening income inequality and negative family environment were noted to be factors [5]. Other changes that may be implicated in mental health problems include increasing exposure to screen time, internet, and social media [13]. Another possible explanation for the increasing trend is the increased readiness to report symptoms due to changes in attitudes and awareness of mental health problems as seen in the review [12].
Majority of the studied population were adolescents or those between the age of 12-18, followed by those between the age of 6-11 (Table 2). This is in line with the systematic review by Bor, et.al. [12], wherein although there was no worsening trend in mental health among toddlers and children, there was note of deteriorating internalizing symptoms in adolescents, that causes greater burden in mental health among the pediatric population [12]. The World Health Organization reports that globally one (1) in seven (7) ten- to nineteen-year-old experiences a mental disorder which accounts for 13% of the global burden of disease in this age group [14]. In the Philippines, 16% of children had mental disorders based on a WHO survey, which approximates the incidence worldwide [15]. Several studies on the epidemiology of psychiatric disorders have its onset during their adolescent periods [5,13]. Major depressive disorders and other depressive disorders, in a longitudinal community study has shown that average age of onset was between 11 and 14 years [13]. For bipolar disorder the incidence peaks at the age of 14 in both male and female [16].
Given that more than half of the cases seen were forensic child abuse cases, that are mostly female, the data may be skewed towards the female sex, which may not give us a clear picture as to the sex distribution of primary psychiatric disorders. Nevertheless, the data put into light that female children may be at an increased risk for psychiatric disorders because of their preponderance to abuse. However, in a national baseline study by Ramiro and Luna in 2016, on Violence Against Women and Children (VAWC) in the Philippines, they found that there are more males (51.2%, with a study population of 3,866) who experienced abuse as children. As such, reporting on abuses among male children may be underrecognized, which may be the case in this study [17].
The proximity of provinces in the Davao Region to the psychiatric facility may explain the large number of the studied population coming from this area. Adjacent regions also contributed to the numbers. Geographical location can greatly affect health-seeking behavior and is also true for psychiatric consults. Proximity was noted in a study to be a strong determinant for health seeking [18,19]. This study found that most of the children seen for consultation at the Out Patient Department are enrolled in schools, with 41.9% in elementary level and 43.3% in high school level (Table 2). This corresponds to the age range of the study population wherein children are expected to be enrolled in school. A UNICEF report on the status of children in the Philippines noted that in 2015, the net enrolment rate in primary education was 91.05% while there was only 68.15% in secondary school [20]. This may explain why there were only 43.3% of the study population were in high school as compared to the 64.4% who were at the age of 11-18.
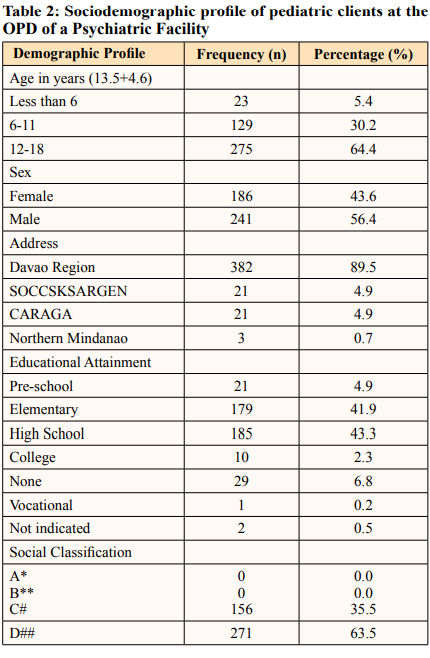
*per capita income of > Php 100,000 ** per capita income of Php 50,000 to 99,000 # per capita income of Php 15,001 to 50,000 ##per capita income of below Php 15,000
The psychiatric facility mainly caters to patients belonging to the lower income groups. Majority of the study population belongs to the social class D which are families who have per capita income of less than Php 15,000. However, this number may be affected by the large number of the study population coming in for forensic reasons, wherein they were immediately classified under social class D and were being given free services.
The increased percentage of the study population diagnosed to have Adverse Childhood Experience and trauma-related disorders (Table 3) parallels results in a systematic review by UNICEF where data showed that more than half of the children worldwide experience abuse, and 64% of these abuses are in Asian countries
[21]. The high reporting of abuse cases may be explained by the active programs of the government in protecting children specifically in Davao City. The data highlights the necessity of continued linkage with child protection institutions.
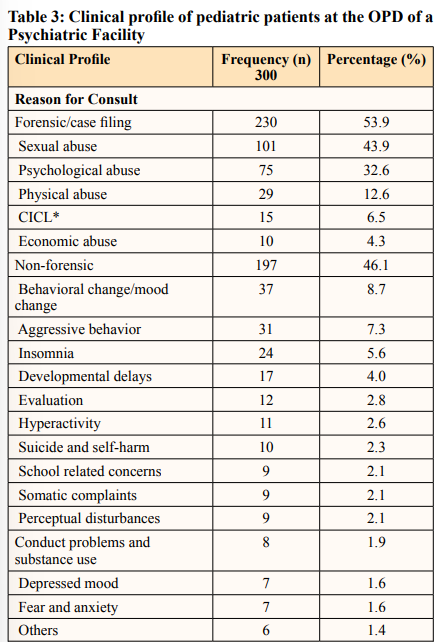
The high frequency of children and adolescents with adverse childhood experiences noted in this study could be at risk of having developmental and mental health outcomes and a wide range of personality-psychological disorders that include behavioral disorders, mood disorders including suicide among others. Various studies have also linked abuse and trauma in childhood as risk factors to developing psychiatric disorders and substance use in adulthood [22-24].
Several points can be drawn from the data. First, of the 14.8% seen to have neurodevelopmental disorders, only less than 1% were referred to Occupational Therapy which is a possible gap in the service utilization for this population. Furthermore, while there was a high percentage of children referred to psychological services, this may be in large part due to the high percentage of forensic cases, and the increase may be in parallel to the increased need for Neuropsychological Testing, as a requirement for psychiatric evaluations for forensic reports.
The study documented 10.3% of consults were diagnosed to have psychotic disorders. Worldwide, the incidence of psychotic disorders in children can be as high as 7.9% to 14% [25,26].
Mood disorders comprised 4% of the study population. Anxiety and depressive disorders were reported globally to be the most prevalent psychiatric conditions in the 10 to 19 age group [14]. While in a population survey for mental disorders conducted from 1993 to 1994 by the University of the Philippines’ Psychiatric Foundation which was conducted in three underprivileged urban and rural provinces showed the prevalence of mood disorders at 1.1% [27].
Majority of the study population was catered as Outpatient which may have been influenced by the increased number of forensic consults.
The sociodemographic and clinical profile of child and adolescent patients was investigated in this study. The number of child and adolescent consults in the outpatient department of the psychiatric facility steadily increased within the span of five years. The study showed that there were more teens who consulted at the outpatient department. Other sociodemographic that were described in this study showed that more teens, females who were from Davao Region, belonging to the class D social classification consulted in the institution. The results further showed that more than half of consults were forensic in nature with almost half as alleged victims of sexual abuse. A third of the consults were diagnosed to have Adverse Childhood Experiences.
There is a gap in the data as to the outcome of the study population seen for both forensic and non-forensic cases. Further research could be done in exploring the barriers to access and service utilization of mental health programs in the region. The results will be valuable information to steer policy making and program implementation to services that will cater to children who had adverse childhood experiences or drafting policies to prevent such events from occurring.