Author(s): <p>Anurodh Kumar, Chandrashekhar Gendle and Sushanta K Sahoo*</p>
Penetrating brain injuries due to sharp knife are low velocity trauma but need urgent surgical intervention. We discuss a 28-year COVID positive male with left supra orbital penetrating brain injury with a sharp knife. Radiology showed the object entered through the left frontal bone near the key burr point. Reconstructed CT images showed the entry point close to the sylvian fissure and the trajectory was away from it. Craniotomy was done leaving a rim of bone around the knife, dura opened, sylvian veins were seen and the knife was gently pulled out without any additional injury. The patient recovered without any complication. Proper preoperative evaluation and surgical planning is essential in extraction of sharp objects in cases of penetrating brain injuries.
Penetrating brain injury by sharp knife is unusual. These are low velocity trauma but may have severe consequences secondary to injury to major vessels. Surgical removal of the sharp object without additional injury is important [1, 2]. We discuss here a 28-year male who operated for an injury with a sharp knife that entered through the left supraorbital area. The preoperative planning and operative steps are highlighted.
A 28-year male presented to our trauma emergency with alleged history of trauma with a sharp knife during violence. On examination he was conscious, oriented without any focal motor deficit. Local examination revealed a metallic foreign body at the left supra orbital area. Part of the foreign body had pierced the skull bone and fixed at that point. He was planned for surgical removal of the foreign body. Considering the ongoing COVID-19 pandemic, he was screened in the preoperative period. The RT-PCR for SARS COV-2 was positive and the patient was immediately shifted to the COVID care center. Non contrast computed tomogram showed a sharp foreign body piercing through the left frontal bone in to the brain matter. There was no hematoma seen along the foreign body tract, no extradural or subdural collection. 3D reconstructed images showed the foreign body has entered through the frontal bone just above the key point and is perpendicular to the coronal plane [Figure 1].
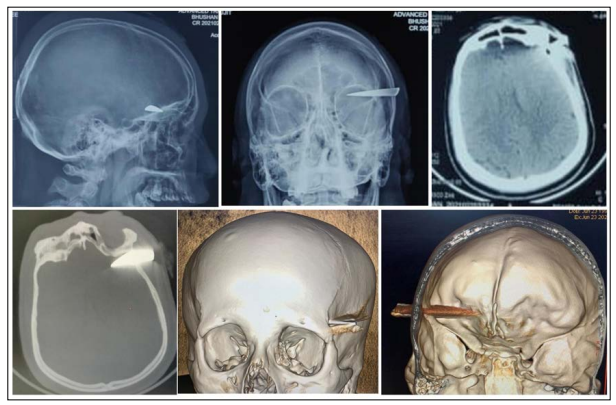
Figure 1: A&B: X-ray showing sharp foreign body in the left supra orbital area. C& D: NCCT head showing foreign body in the left frontal area. Note there is no hematoma in the brain parenchyma. E&F: 3D reconstructed CT images showing the foreign body entering close to the left key burr hole area and passing perpendicular to the coronal plane parallel to the floor of orbit.
A fronto temporal flap around the foreign body was raised. Wide craniotomy was done, suspecting brain edema and four burr holes at the corners were made. Then a bony gutter was made around the foreign body with the help of rongeurs without disturbing the metal piece. Then the craniotomy was performed with gigli saw wire. The bone flap was elevated carefully leaving behind the small piece of bone around the metal piece. As the foreign body was sharp and the entry point was close to the sylvian fissure, blind pulling of the foreign body was avoided. Dura was opened and sylvian veins were seen away from the foreign body [Figure 2]. Then the metal piece was gently pulled out and the tract was inspected for any bleeding. The retrieved foreign body was a piece of knife with sharp pointed tip. After hemostasis wound was closed and the patient was kept on anti epileptics and antibiotics. Post operative CT showed small bleed in the frontal region along the tract. The patient recovered well and there was no peri operative complication.
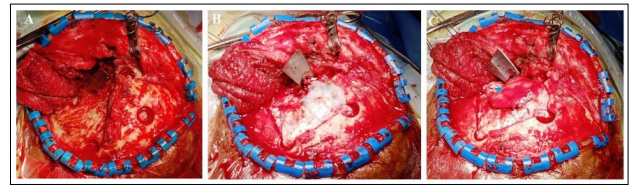
Figure 2: A&B: Intra operative image showing position of burr holes around the foreign body. C: sylvian vessels (blue star) seen away from the foreign body
Penetrating head injuries may be due to high velocity or low velocity trauma. Most of the high velocity head injuries occur at the warfare due to missile or bullets. Low velocity penetrating brain injuries are noticed at domestic violence with sharp metallic objects [3]. Injury due to a sharp knife is less common.
Usually these are stabbed by another person, self inflicted and less commonly by accident [4]. As the sharp end of the knife pierces the skull bone, maximum energy dissipated at the bony entrance and the object enters the brain parenchyma with less energy. Therefore, they may not produce major parenchymal damage. However, injury to the blood vessels or sinuses may result in massive hemorrhage and have a poor outcome. Apart from this there may be associated subdural/epidural hematoma. Urgent CT scan gives an idea of the type of bleed and if necessary angio should be done to exclude traumatic pseudoaneurysm or aretriovenous fistula [1]. As our patient turned COVID positive, with limited resources in the COVID care center, angiogram could not be performed. Moreover, there was no underlying hematoma to suggest vascular injury. Early surgical intervention is essential as wound site infection may lead to brain abscess.
Surgical removal of the sharp knife from the brain parenchyma is tricky. A sudden jerky movement may result in injury to the adjacent vessels as in our patient it was close to the sylvian fissure. Location of entry wound and the entire trajectory should be thoroughly reviewed on radiology. At times a 3D reconstructed image with multiple cut sections in different planes gives a clear picture of the sharp object in relation to vital structures of brain. In our patient the entry was just adjacent to the key burr hole point and the knife had traversed perpendicular to the coronal plane along the orbital roof. Radiologically the entry was close to the sylvian fissure but the trajectory was anterior to it. As the entry was close to the veins, we left a small rim of bone around the knife while making the craniotomy. We considered dural opening prior to removal of the foreign body to look for the sylvian veins in relation to the lodged knife. The cortical vessels were visualized and preserved while removing the knife. Sudden puling of the sharp knife close to major vessels will have a risk of injuring them and should be avoided (Table 1).
Penetrating brain injury with sharp knife is rare and need early surgical intervention. Pre operative radiology should be evaluated thoroughly to look for the trajectory of the foreign body when it is close to important major vessels like sylvian veins.