Author(s): Djiguiba K*, Doumbia M, Toure M, Coulibaly A, Kodio A, Sy S, Fongoro S, Benamar L, Ezaitouni F, Bayahia R, Ouzeddoun N and Yattara H
Introduction: Renal infraction is a rare medical-surgical emergency that should be evoked before any lumbar pain syndrome. We report in this work, two cases of renal infraction with their clinical evolution.
Clinical observation: These patients, aged respectively 48 and 70 years, were hospitalized in our department concomitant for low back pain. Emboligenic heart disease was responsible for the renal infraction in both cases. Diagnostic certainty was established by a CT scan with injection of contrast medium. Renal function was normal in the young patient versus renal insufficiency at 20mg/l creatinine for a GFR estimated at 35ml/minute according to MDRD in the elderly patient. We had a clinical and biological improvement with a curative anticoagulant treatment relayed by a long term treatment with an anti vitamin K in both cases but the elderly man kept a sequential renal insufficiency.
Conclusion: Acute renal infarction is a rare pathology which must be systematically evoked in front of a lumbar pain syndrome. Angioscan with injection of contrast medium allows to make the diagnosis. Heparinization at an effective dose is the mainstay of treatment in the case of unilateral involvement, or surgery if bilateral.
Renal infarction is a rare pathology that must be evoked before any lumbar pain syndrome. It constitutes a medical and surgical emergency. In order to better preserve renal function, any acute occlusion of the renal artery or one of its branches, whether partial or total, must be diagnosed as soon as possible. A delay in diagnosis beyond 3-4 hours leads to irreversible parenchymal lesions, the functional consequences of which can be serious. Despite the development of advanced radiology techniques, the diagnosis of renal infarction is often delayed or even missed. Although the first case of renal infarction has been described since 1865, its incidence is currently unknown. It is an entity that is generally ignored by clinicians because these symptoms may suggest acute pyelonephritis or even renal lithiasis or acute appendicitis. The most frequent causes are related to an emboligenic cardiac pathology [1, 2]. Through these 2 cases, we will discuss the clinical characteristics, the diagnostic and therapeutic approach, and the clinical evolution, and a review of the literature.
Z.K, patient 48 years old is followed since 2002 for ischemic heart disease and dyslipidemia. He was admitted to the nephrology department for left nephritic colic. His blood pressure is 140/60 mmHg, and the somatic examination is normal except for an irregular heartbeat and left lumbar pain on palpation. Diuresis is preserved. Serum creatinine is 9 mg/l with a normal urine sediment. CRP was 165mg/l and CBC showed hyperleukocytosis at 17900/mm3 with predominantly neutrophils without anemia (Hb = 15 g/dl). The level of lactic dehydrogenase (LDH) was increased to 813 IU/l. The immunological work-up (ANCA; anti DNA; anti MBG; APL) was negative. Serum complement fractions C3, C4 are normal. The ECG did not show any particularities. An abdominopelvic computed tomography (CT) performed on D?? of his admission showed a partial infarction of the left renal parenchyma, superior polar and inferior polar evoking segmental emboli; the renal artery and renal vein were free (Figure 1(a)).
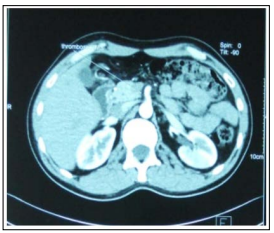
Figure 1(a): An Angioscan of the Abdomen: A Partial Infarct of the Left Renal Parenchyma, Upper Polar and Lower Polar
The superior mesenteric artery (SMA) on thoracoabdominal angioscan, the celiac trunk (CT) are the site of a non-occlusive thrombus (Figure 1(b)). On trans-thoracic cardiac echocardiography (TTE) the diastolic function is impaired, the basal and medial segment of the septal wall as well as the lateral wall segment are the site of hypokinesia. The patient was put on an anticoagulant, an inhibitor of the conversion enzyme, a beta blocker and a statin. At 2 months of evolution, the renal function is still stable (creatinine at 8.1mg/l), the CRP at 4mg/l but the hyperleukocytosis persists at 16000/mm3 and the LDH have regre.
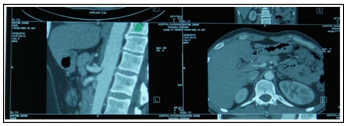
Figure 1(b): Angioscan of the Abdomen: Showing Thrombus in the Superior Mesenteric Artery and Celiac Trunk
B.B, 70 years old, known hypertensive for 30 years, presented to the nephrology department. For intense right lumbago with fever at 38°c without hematuria, nor mictional burning. His blood pressure was 120/80 mmHg and cardiac auscultation showed an irregular rhythm, related to an ACFA on the ECG, on which there was also posterior inferior necrosis, subendocardial and anteroseptal ischemia.
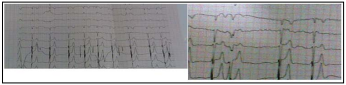
ECG electrocardiogram: ACFA and Posteroinferior Necrosis, Sub EndoCardial and AnteroSeptal Ischemia
Palpation of the right lumbar region did not reveal any mass. Biologically, the patient presented with renal failure (serum creatinine at 20mg/L with clearance according to the MDRD formula = 35ml/min. The 24-hour proteinuria is 0.71g/24h with preserved diuresis. No leukocyturia, no hematuria, no urinary infection. CRP was 246 mg/l, and leukocytosis was 16500/mm3, predominantly neutrophils. LDH was increased to 636 IU/l. The C+ renal CT scan showed a nephrographic defect involving almost the entire right kidney (Figure 2).
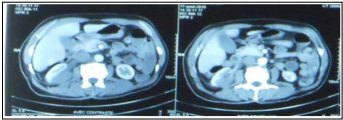
Figure 2: Renal Angiocanner C: shows a Nephrographic Defect Involving almost the Entire Right Kidney
Trans thoracic echocardiography (TTE): Found biauricular dilation and dilated right chambers with a systolic ejection fraction of 45% and abnormalities of segmental kinetics. The patient was put on anticoagulation, followed by an anti vitamin K, a statin and an ACE inhibitor. After ten days of evolution the pain disappeared, the renal function remained stable and the CRP was reduced to 17 mg/L.
These two observations are similar in several respects: both cases involved the revelation of a renal infarction of cardiac origin in a young and an elderly subject. Renal infarction is a medical-surgical emergency that is rare and affects all ages and both sexes. In an autoptic series of 14400 observations, renal infarction was demonstrated in 205 cases (1.4%), but diagnosed during the patient’s lifetime in only 2 cases [1]. Renal infarcts have a polymorphic clinical presentation without very specific signs: abdominal and/or flank pain, fever or feverishness, oliguria or even proteinuria, and/or hematuria and/or leukocyturia on dipstick, and these signs can be confused with acute pyelonephritis. The variability of the symptoms can explain in part the difficulty of the diagnosis. Pain is the first symptom in 80-90% of cases, but sometimes pain is absent. It can be assumed that a significant proportion of renal infarctions are asymptomatic or undiagnosed. The etiologies are dominated by emboligenic heart disease in 94% of cases, cholesterol crystal embolism, venous thrombosis with paradoxical embolism, vasculitis, Takayashu, syphilis [2,3]. Some authors have incriminated cannabis use [4,5]. On the biological level, a clear and persistent elevation of LDH. This elevation of LDH is explained by the renal parenchymal necrosis. Often a high blood pressure may accompany the clinical picture, if present it certifies the release of angiotensin, a powerful vasoconstrictor hormone [6]. The diagnosis is made by angioscan with injection of contrast medium, and also arteriography. Standard ultrasound is not contributory, it allows to eliminate lithiasis, just to have the size of the kidneys, the presence of possible obstruction [4]. TC 99 scintigraphy allows to highlight the large infarcts [7,8]. The treatment of renal infarction is a controversial subject, because there is no consensus it must be decided in a multidisciplinary way between the nephrologist and the vascular surgeon. Some authors report a significant mortality of the surgery. If the damage is unilateral the treatment of choice is anti coagulation and if bilateral the choice is surgical but no difference. The success rate between surgery and medical treatment varies between 75-80%. However, it should be noted that surgery has no place in intra parenchymal vascular occlusions [9,10].
Acute renal infarction is a rare pathology that must be systematically evoked in front of a lumbar pain syndrome. Angioscan with injection of contrast product allows the diagnosis to be made. Heparinization at an effective dose is the mainstay of treatment in the case of a unilateral attack, or surgery if bilateral.