Author(s): Ashok Garg, Deepak Agrawal*, Deepika Mishra and G L Sharma
A Patent Foramen Ovale (PFO) is not a true deficiency of atrial septal tissue but rather a potential space or separation between the septum primum and septum secundum located in the anterosuperior portion of the atrial septum. It is not considered a true Atrial Septal Defect (ASD), because no structural deficiency of the atrial septal tissue is present. We are describing a unique case of recurrent transient attacks followed by stroke associated with finding of a large stretched PFO on echocardiography.
A 43-year-old woman presented with a complaints of right upper and lower limbs weakness with aphasia since 1 day. She had history of similar episodes 4 times in last 1 year which recovered in less than 1 hour suggestive of transient ischemic attack (TIA). She did not consult to any physician for past complaints because symptoms were abated self without any treatment. Currently her weakness was persistent and she was unable to speak, therefore she sought physician consultation.
She had no history of any breathlessness, headache or vertigo in past. There was no past history of any chronic disease. On examination her blood pressure was 124/80 milimeter of mercury and pulse was 74/ minute and regular. ECG done which showed normal sinus rhythm. As per neurologist opinion for stroke and aphasia, her MRI brain was done which revealed left middle cerebral artery territory infarct in frontoparietal lobe with old lacunar infarct in right cerebellar hemisphere. She was referred to us for echocardiography. A two-dimensional transthoracic echocardiography was done with a Vivid S5 GE (Milwaukee, Wisconsin, USA) ultrasound system with a 3 MHz transducer. It showed situs solitus of the atria, atrioventricular concordance, d loop ventricles and ventriculo-arterial concordance. A moving flap of interatrial septum was seen intermittent left to right shunt. We suspected it as a PFO. Thereafter agitated saline contrast study was performed. The saline injected in right antecubital vein which shows the bubbles in right atrium and right ventricle and minimal saline bubble in left side of heart passing through this defect. For further confirmation about the defect, transesophageal echocardiography (TEE) was performed which revealed a space between the septum primum and septum secundum located in the anterosuperior portion of the atrial septum (Figure A, supplementary video 1). There was no true anatomical defect of the atrial septal tissue. On colour Doppler echocardiography there was a large shunt from left to right atrium (Figure B, supplementary video 2). TEE findings confirmed the presence of stretched patent foramen ovale (PFO) and it was further confirmed during surgery for PFO. Surgery was performed through right minithoracotomy and size of PFO was found as 35 mm, which was closed successfully. On follow up visits, patient is doing well and there is no episode of TIA or stroke.
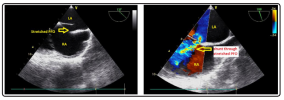
Figures A & B: showing transesophageal images of stretched PFO and left to right shunting
Transesophageal echocardiography showing a stretched patent foramen ovale
Transesophageal echocardiography showing a stretched patent foramen ovale and left to right shunting through it
The association of PFO and stroke was first described in 1877 by Julius Friedrich Cohnheim. Cohnheim hypothesized that a torn-off piece of thrombus arising from lower extremity traveled to the right atrium into the left atrium and to the frontal lobe [1]. Approximately 25% of the adult population has a PFO but this condition by itself has not been associated with the increased risk of ischemic stroke [2]. Although the prevalence of PFO is significantly higher in patients with cryptogenic stroke; up to 40% of ischemic strokes without an identifiable cause have a PFO [3]. It implicates the role of paradoxical embolism through a PFO in cryptogenic strokes.
A PFO is not a true deficiency of atrial septal tissue but it is a potential space between the septum primum and septum secundum located in the anterosuperior portion of the atrial septum [4]. It is not considered a true atrial septal defect (ASD), because no structural deficiency of the atrial septal tissue is present. When a PFO is stretched open by atrial hemodynamics, thus creating a defect in the septum, it is referred to as a ‘‘stretched’’ PFO. This can result in left to right or right to left shunting of blood flow demonstrated by Doppler, depending on the differences in the right and left atrial pressure.
Stretched PFO is a rare entity reported in literature. A case report was published in British medical journal in 2012 describing the development of platypnea-orthodeoxia syndrome secondary to the development of right to left shunting through a ‘stretched’ PFO [5]. Our patient had recurrent transient attacks followed by stroke and it was associated with finding of a large stretched PFO on echocardiography. This case is a unique presentation of stretched PFO in association of stroke.