Author(s): Munazzah Aziz
To determine the frequency of seroma formation after flap fixation by quilting technique in MRM patients as compared to control group.
Study Design: Randomized controlled trial.
Seroma formation, with an incidence of 25-60%, is one of the most common and troublesome consequence of Modified Radical Mastectomy for breast carcinoma [1].
Clinically significant seroma formation causes pain, discomfort, skin flap necrosis and wound dehiscence. In addition to causing anxiety, seroma formation predisposes patients to frequent aspirations and increases the risk of surgical site infections which also delays the start of adjuvant therapy [2].
Multiple factors affecting seroma formation include extent of axillary dissection, presence of dead space after wound closure , use of sclerosants, pressure garments, post operative physiotherapy and body mass index of patient [3].
Ideal wound closure after MRM focuses primarily on meticulous hemostasis, ligation of lymphatics and obliteration of the dead space by holding skin flaps securely to the chest wall structures and early removal of fluid as it forms [4].
Conventionally after MRM, the wound is closed in two layers with 3-0 absorbable sutures placed in the subcutaneous tissues, while the skin edges are approximated with staples or with 4-0 absorbable subcuticular sutures [5].
For reducing seroma formation after modified radical mastectomy, several techniques of flap fixation to chest wall have been formulated. Quilting technique involves suturing of the subcutaneous fascia to the underlying pectoralis fascia and closing the axillary dead space [6].
Mostafa A. Sakkary conducted a study from June 2009 till July2010, compared flap fixation in MRM with conventional wound closure. Frequency of seroma formation in flap fixation group was 2/20 vs 7/20 in conventional group (p = 0.028), drain was also removed in significantly shorter time compared to the control group, fifth vs 13th day. (p < 0.001) [7]. Also, the total fluid drained was significantly lower in the flap fixation group524 ml vs 2017ml (p < 0.001) [8].
Britt Ten Wolde concluded in his study that the incidence of seroma decreased from 80.5% to 22.5% in quilted group (p <0.01) . In randomized controlled trial carried out by Ashraf khater from Feb 2012 to 2014, the incidence of seroma was 20% (12/60 patients) in quilting group as compared to 78.3% (47/60 patients) in control group , with a highly significant difference ( p value<0.001) [9].
The rationale of this study was to evaluate the efficacy of quilting of flaps and obliteration of Axillary space during Modified Radical Mastectomy in reducing seroma formation. Local data on the use of this technique is very limited. Adoption of this technique is expected to help in early discharge from hospital, decrease psychological morbidity and early commencement of adjuvant therapy for breast cancer [10].
The objective of the study was:
• “To determine the frequency of seroma formation after flap fixation by quilting technique in MRM as compared to control group.”
Resection of all the breast tissue, nipple areola complex and skin along with removal of level I, II and III axillary lymph nodes.
Pocket of sterile fluid collection under the skin flaps or in the axillary dead space following modified radical mastectomy, apparent as a bulge on skin and confirmed by needle aspiration on 5th Postoperative day
There is decreased incidence of post mastectomy seroma formation in MRM with quilting of flaps as compared to the conventional method of wound closure in MRM.
This randomized controlled trial study was conducted at Department of Surgery, Holy Family hospital, Rawalpindi Pakistan, from 11th November 2017 to 10th May 2018. A total of 60 patients having histologically proven breast cancer stage 2 or 3 undergoing modified radical mastectomy and aged 40-70 years were included. Exclusion criteria involved patients having coagulation disorders, those who had already received neoadjuvant therapy for down staging and chronic liver disease. Patients were allocated to group1 or group2 by random selection. In group I, flap fixation by quilting technique in MRM was done while in group II no quilting was done. Patients were followed up in OPD after 05 days and observed for development of seroma clinically.
After admission, written informed consent was taken for participation in the research project. Patients were allocated to group1 or group2 by random selection. MRM was performed with a standardized technique using monopolar diathermy. In the 1st group, continuous suturing of undersurface of upper flap was done with the pectoralis fascia (medial to lateral) with vicryl 2/0. The second row was done similarly from lateral to medial till the medial edge. Procedure was done in a similar fashion for the lower flap. The lateral wall of axilla was sutured to the fascia of the serratus anterior and medial axillary wall. An 18 French tube drain was inserted in the axilla and flaps in all cases of the study. In the control group, continuous vicryl 3/0 suture was used for closure of the subcuticular layer and dermis in two layers. 18 French tube drain was placed in the flaps and axilla. Surgical wounds were dressed with adhesive dressings. On postoperative day one patients were consulted by physiotherapist for exercises. Drains were removed on second POD. On discharge, patients were provided a mobile number to contact in case of any complication. Patients were seen in OPD after five days and observed for development of seroma clinically and using needle aspiration.
Analysis done using SPSS Version 20. For qualitative variable like frequency of seroma formation, Stage of breast cancer, frequencies and percentages were calculated. Effect modification like age and BMI, stage of Cancer were controlled by stratification. Post stratification chi square test was applied to compare frequency of seroma. Qualitative variables were presented through tables and charts. P value of <0.05 was considered statistically significant.
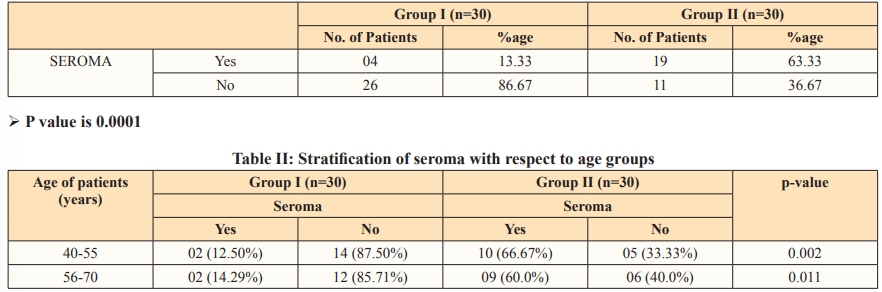
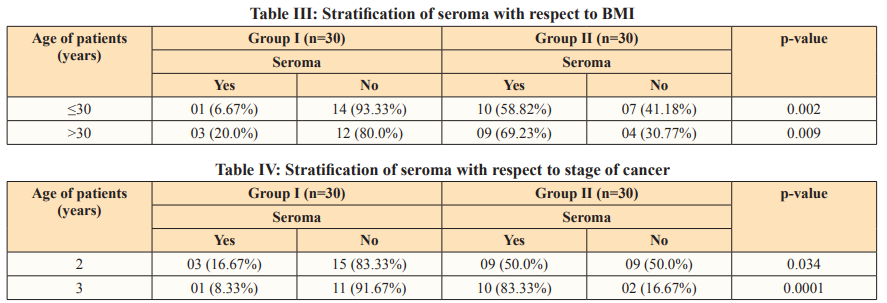
Age range in this study was from 40 to 70 years with mean age of 55.23 ± 7.94 years. Majority of the patients 31 (51.67%) were between 40 to 55 years of age. Mean BMI was 30.05 ± 2.63 kg/ m2. Seroma formation was seen in 04 (13.33%) in group I (flap fixation by quilting technique in MRM) and 19 (63.33%) in group II (control group) with p-value of 0.0001 as shown in Table I. Stratification of seroma with respect to age groups and BMI in both groups is shown in Table II & III respectively.
Breast cancer, being the most commonly occurring cancer in the women worldwide, effects the quality of life of women and needs effective management . The primary surgical cure of breast cancer by modified radical mastectomy leads to a cumbersome complication of seroma formation. Seroma formation has a reported incidence of 3 to 85% after MRM. Collection of seroma and its repeated drainage causes much discomfort to the patients due to repeated hospital visits , local wound complications and a delay in the commencement of adjuvant therapy for breast cancer [11]. Multiple factors lead to seroma formation . The likelihood of developing seroma after breast cancer surgery was 2.5times higher after Modified radical mastectomy in a study by Hashemi et al [12].
Gonzalez et al. also interpreted that the extent of surgical resection is a strong predictor of seroma development by comparing seroma formation after wide local excision and modified radical mastectomy [13]. Another factor associated with seroma formation is electrocautery dissection. Electrocautery dissection causes an increased inflammatory response in the wound leading to increased seroma formation as compared to scalpel dissection [14]. Although seroma formation cannot be completely avoided at present but a metaanalysis of 136 studies shows that surgical closure of dead space after mastectomy can reduce seroma formation [15].
Routine usage of drains for extended duration and use of bandages/ pressure garments for external compression are a conventional practice but they have not proven to be of significant benefit in reducing seroma formation. These techniques are troublesome to the patient due to prolonged hospital stay, repeated hospital visits for seroma aspirations, surgical site infection, poor cosmetic outcome and consequently increased financial burden to the patient. Almond et al concluded in his study that surgical flap fixation techniques can be an economical alternative to drain placement with comparable seroma formation rates but reduced hospital stay [16]. Suture flap fixation by quilting resulted in a significantly lower frequency and amount of seroma formation in comparison to conventional method of wound closure in a trial by Mostafa A Sakkary (p = 0.028)7
n our study, mean age of patients was 55.23+/- 7.94years. Mean body mass index of the patients was 30.5+/_2.63kg/m2 . Seroma formation was seen in 13.33% patients in flap fixation group and in 63.33% patients in the control group with a p-value of 0.0001. The extent of the dissection plane seems to be an important factor in seroma formation, and therefore, obliteration of dead space in patients undergoing mastectomy or modified radical mastectomy seems to be pivotal. Pressure garments or compression bandages are not effective in combating seroma; however, quilting of the skin flaps seems to be much more effective [17].
In a similar study by James Van Bastelaar conducted in Netherland, 188 patients were included , 33/92 (35.9%) patients developed seroma in flap fixation group while 52/88(59.1%) patients developed seroma in the control group (p=0.002). Moreover seroma aspiration rate was also lower in the flap fixation group (p<0.001) [18].
In an another prospective cohort study conducted in Norfolk and Norwich University Hospital, 168 patients undergoing mastectomy were recruited with 54 in quilting group and 114 in nonquilting group. 29% patients in the quilting group developed significant seroma necessitating aspiration and 69% in the nonquilting group (p<0.001) [19].Thus we propose that routine use of quilting technique during mastectomy can have a positive effect on patients recovery and decrease the discomfort related to seroma formation.
This study concluded that there is decreased incidence of post MRM seroma formation with quilting of flaps as compared to the conventional method of wound closure in MRM. So, we recommend that quilting of flaps should be used routinely after modified radical mastectomy in order to reduce the incidence of post mastectomy seroma formation.