Author(s):
Background: Pervasive developmental disorders include five chronic disorders marked by early impairment in socialization, communication and behavior. Little is known about the types of pervasive developmental disorders in Iraq. This is a retrospective clinical study aiming at determining the types of pervasive developmental disorders in Iraqi children observed at the pediatric psychiatry clinic in a tertiary pediatric referral center. Patients and Methods: During nine months period (November 18th, 2018 to July 18th, 2019), fifty one patients with a diagnosis of pervasive developmental disorders (30 males and 21 females) were observed at the psychiatry clinic at the Children Teaching Hospital of Baghdad Medical City. Their ages ranged from two and half years to twelve years. Results: Thirty two (17 males and 15 females) patients had autism without significant mental retardation as indicated by adequate urine and bowel control and self care skills particularly spoon feeding. Thirteen patients were considered to have atypical autism or Pervasive developmental disorder not otherwise specified (10 boys and 3 girls), in eleven of them, the disorder was considered atypical because of the lack of adequate urine and bowel control and self care skills particularly appropriate spoon feeding indicating significant degree of mental retardation. In one patient, his condition was considered a typical because of the presence of an acceptable eye contact and response appropriately to name in most instances. Three patients had Asperger syndrome including two girls and one boy. Two boys had childhood disintegrative disorder (Heller syndrome), one of them have changes on brain MRI suggestive of cerebral vasculitis. One girl had Rett syndrome and her case and early treatment was published. Conclusion: In this series, typical autism without significant mental retardation accounted for 63%. Atypical autism (Pervasive developmental disorder not otherwise) was the second most common type of Pervasive developmental disorders accounting for about 25%. Asperger syndrome accounted for only 6% of the cases in this series
The term pervasive developmental disorders was probably first used during the 1980s. Pervasive developmental disorders include five chronic disorders marked by early impairment in socialization, communication, and behavior [1,2].
These disorders were first recognized by Grunya Efimovna Sukhareva in 1925, a Soviet pediatric psychiatrist who called these disorders autistic psychopathy. In general, most of manifestations of pervasive developmental disorders result from impairments in social interaction and communication and behavioral problems [1,2,3].
Autistic Disorder: which is also called typical autism was first described by Leo Kanner in 1943[1].
Asperger Syndrome: It was first described by Grunya Efimovna Sukhareva and later by Hans Asperger in 1944[1].
The autistic psychopathies described in 1925 by Grunya Efimovna Sukhareva and Hans Asperger were similar and characterized by the absence of significant impairment in language development and cognitive function. Lorna Wing was probably the first to use the term Asperger syndrome in the English-speaking medical community in her 1981 publication of a series of case studies of children showing similar symptoms. Uta Frith translated Asperger’s paper to English in 1991 and published it as a book with Cambridge University Press [1,2].
Asperger syndrome became a standard diagnosis in 1992, when it was included in the tenth edition of the World Health Organization’s diagnostic manual, International Classification of Diseases (ICD-10); in 1994, it was added to the fourth edition of the American Psychiatric Association’s diagnostic reference, Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) [1,4].
The World Health Organization (WHO) defined Asperger syndrome as one of the pervasive developmental disorders or autism spectrum disorders which are a variety of psychiatric conditions that are characterized by impairment of social interaction and non verbal communication, and by restricted and repetitive interests and behavior[1,2].
Rett Disorder: It was most probably first described in German language in 1966 by Andreas Rett (Figure-6), a pediatrician in Vienna. Bengt Hagberg, a Swedish pediatrician, published an English article in 1983 and named the condition after Rett [5,6].
Childhood Disintegrative Disorder (Heller Syndrome): It is a rare heterogeneous clinical syndrome that is distinctive from autism and Asperger syndrome. It is characterized by a significant developmental regression resulting in deterioration in behavioral and adaptive functioning including self-help skills with loss of language and social skills after a period of normal development for at least two years [6].
The condition was first reported in 1908 by Theodor Heller in his paper “über Dementia Infantilis”. He called the condition “Dementia infantilis”.
Pervasive Developmental Disorder not Otherwise Specified (Atypical Autism): This type reflects the marked variability of these disorders. It may include disorders with a well defined clinical features such as regressive autism and autism with significant mental retardation which seems to be also classifiable under idiopathic mental retardation with significant autistic features [1,2,6].
Regressive autism is just like Heller syndrome, it is associated with initial normal development followed by loss of the previously acquired skills of socializing, communication and language skills. However, regressive autism is not associated with features of dementia or significant mental retardation [1,6].
Pervasive developmental disorders has recently been called autism spectrum disorder mostly by the american psychiatric association and the term pervasive developmental disorders has been used with the term autism spectrum disorder interchangeably [1,2]. This is a retrospective clinical study aiming at describing the pattern of pervasive developmental disorders in Iraqi children observed at the pediatric psychiatry clinic in a single tertiary pediatric referral center.
Patients and Methods: During nine months period (November 18th, 2018 to July 18th, 2019), fifty one patients with pervasive developmental disorders (30 males and 21 females) were observed at the neuropsychiatry clinic at the Children Teaching hospital of Baghdad Medical City. Their ages ranged from two and half years to twelve years.
Most of the patients were from the province of Baghdad, but it was documented that there were four patients from other provinces (Najaf, Wassit, Kerbala and Erbil in the North of Iraq).
All the patients had very poor speech development except three patients with Asperger syndrome. Most of the patients with a diagnosis other than Asperger syndrome were not saying any word and few patients were saying few words.
The patients were treated with individualized treatment plans including intramuscular cerebrolysin as the main therapy based on our published experience with treatment of pervasive developmental disorders [8].
Treatment aimed at improving the cardinal features of pervasive developmental disorders which is the impairment of social interaction which is mostly manifested by poor responsiveness to own name and infrequent engagement with others manifested by poor eye contact and infrequently looking at faces.
Most patients also required neuroleptics to control hyperactivity and other abnormal behaviors. Trifluoperazine and prochloperazine were used as necessary. Risperidone was also used sometimes as necessary.
Many patients also received citicoline as an adjunctive therapy to improve speech development.
It is expected that improving social interaction will contribute to improving other features especially verbal communication and speech.
Courses of intramuscular cerebrolysin were given in individualized regimen depending on the age and severity of the illness and with aim of improving social interactions including response to own name, looking at faces and eye contact.
Results and Discussion: Thirty two (17 males and 15 females) patients had autism without significant mental retardation as indicated by adequate urine and bowel control and self care skills particularly spoon feeding. Four boys were considered to have a severe form of the disorder, one of them, the parents thought the child was deaf and consulted initially an ear specialist. One boy had prominent echolalia.
Figure-1 shows an eight-year old boy with severe autism and had significant behavioral abnormalities. He was not saying any word. At the clinic, he was unable to sit still on the chair without frequently changing the position of his body. He also displayed marked repetitive behavior at the clinic.
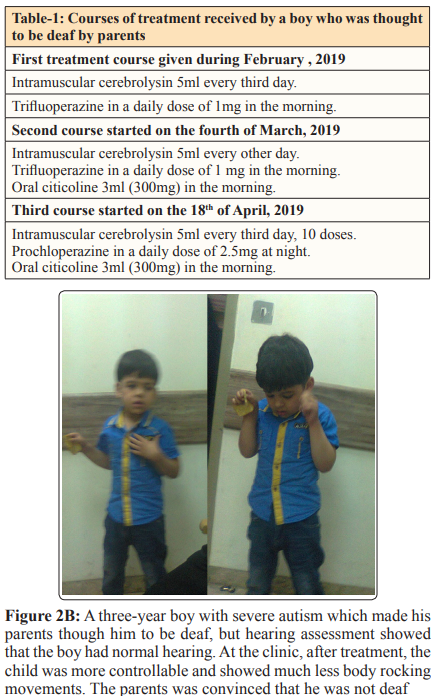
Figure-2A shows a three-year boy with severe autism which made his parents though he to be deaf, but hearing assessment showed that the boy had normal hearing. At the clinic the boy was rather uncontrollable, and displayed marked repetitive movements in the form of body rocking and was trying to leave the room.
Three courses of treatment (Table-1) produced enough improvement to convince the parents that the child was not deaf. At the clinic, after treatment, the child was more controllable and showed much less body rocking movements (Figure-2B).
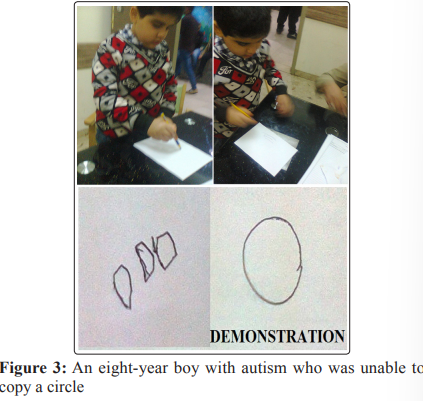
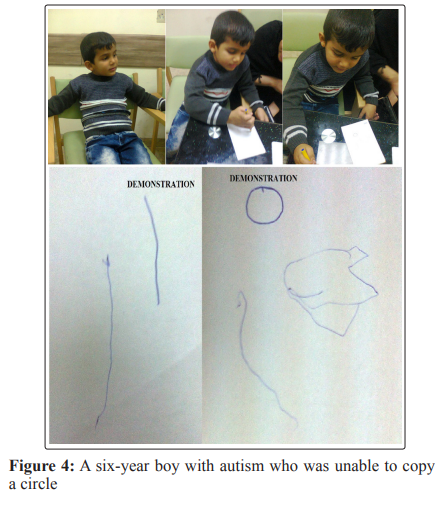
The patients in this group didn’t have significant mental retardation and were classified as having rather typical autism, but most of them had developmental delay particularly in fine motor skills, and had some cognitive impairment manifested by their inability to copy forms.
However, the serious lack of communication skills per se is expected to prevent or delay the acquisition of such developmental mile stones. Figures 3 and 4 shows an eight-year boy and a sixyear boy with autism who were unable to copy a circle.
Thirteen patients were considered to have atypical autism or Pervasive developmental disorder not otherwise specified (10 boys and 3 girls), in eleven of them, the disorder was considered atypical because of the lack of adequate urine and bowel control and self care skills particularly appropriate spoon feeding indicating significant degree of mental retardation. In one patient, his condition was considered atypical because of the presence of an acceptable eye contact and response appropriately to name in most instances.


Figure 2A: A three-year boy with severe autism which made his parents though him to be deaf, but hearing assessment showed that the boy had normal hearing. At the clinic, before treatment, the boy was rather uncontrollable, and displayed marked repetitive movements in the form of body rocking and was trying to leave the room
Six patients (five boys, and one girl) were considered to have a severe form of the disorder. At the clinic, one of the boys with severe disorder was behaving as if he was absolutely not seeing or hearing the doctor for more than five minutes.
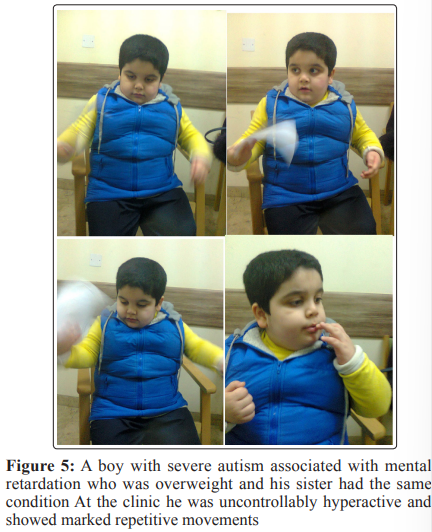
One boy with severe condition was overweight (Figure-5) and the mother thought that his sister had the same condition, but she couldn’t brought her for consultation because the parents were divorced and the girl was under the care of her father. At the clinic the boy was uncontrollably hyperactive and showed marked repetitive movements.
An other boy with atypical autism had infantile left hemiplegic and seizures and another boy had small ventricular defect during infancy. A four and half year’s girl had brain arachnoid cyst on CT scan and MRI. Brain CT-scan at the age of four years showed right anterior basal temporal small arachnoid cyst (23 X 7 X 16 mm). CT-scan also showed that the cisterna pontis and C-P cisterns were prominent on both sides with low density. The CT-scan report also suggested the possibility of epidermoid cyst. Brain MRI confirmed the presence of a right anterior basal temporal (24 X 8 X 17 mm) with clean CSF. MRI also showed atrophic changes of the right temporal lobe.
One boy with atypical autism developed insulin dependent diabetes mellitus. A five-year old girl was considered to have the mildest disorder among patients with typical and a typical autism (Figure-6). Although she didn’t have eye contact and was not responding to calling her time, she was sometime answering questions like how are you and was responding to request of the doctor with the encouragement of her parents.
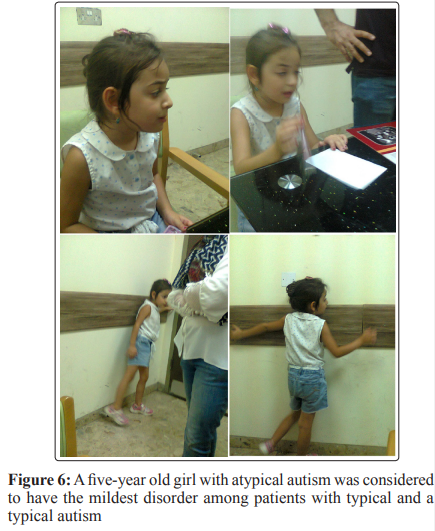
She accepted the doctor request to take a pen, but she couldn’t copy anything. She also had the higher vocabulary of all patients with autism of about 25-30 words, and she waved goodbye when the mother asked her to wave goodbye when leaving.
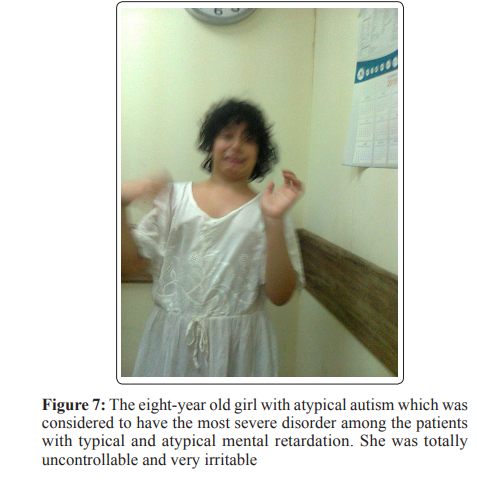
Figure-7 shows the eight-year old girl with atypical autism which was considered to have the most severe disorder among the patients with typical and atypical autism. She was totally uncontrollable and irritable.
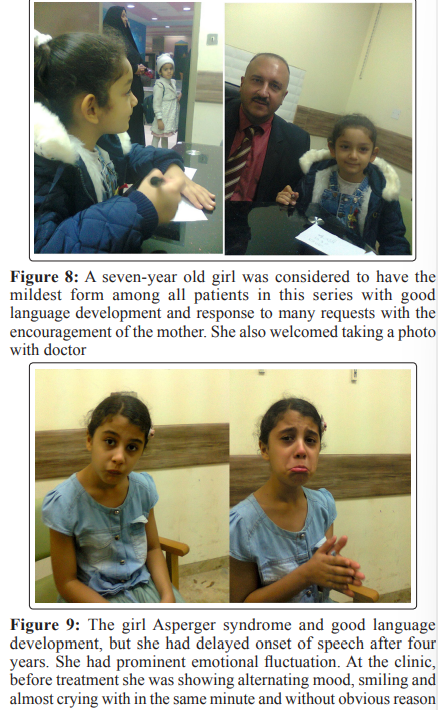
Three patients had Asperger syndrome including two girls and one boy. A seven-year old girl was considered to have the mildest form among all the patients (Figure-8) in this series, with good language development and response to many requests with the encouragement of the mother. She also welcomed taking a photo with doctor. However, her social interaction was impaired as she was not responding appropriately to her name and was not showing acceptable eye contact.
A nine years old girl with Asperger syndrome and good language development, but she had delayed onset of speech after four years. We think that this patient represent a variant of Asperger syndrome with late onset development of language can initially misdiagnosed as a case of autism.
Her measured IQ test ranged from 85 t0 110. She left school because of poor social interaction and communication and emotional fluctuation. At the clinic, she showed alternating mood, she was smiling and almost crying with in the same minute and without obvious reason (Figure-9A). Initial treatment included:
Intramuscular cerebrolysin 5 ml daily for 10 days. Oral trifluoperazine in a daily dose of 1 mg at night. Oral prochloperazine 5mg in the afternoon. After 10 days of treatment, her behavior and emotional swinging improved (Figure-9B). She became rather passionate and when leaving she insisted on hugging the doctor and kissing him.
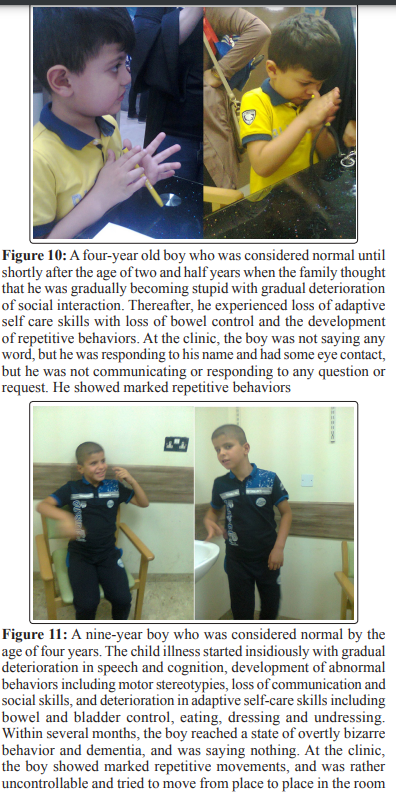
Two boys (Figures 10 and 11) had childhood disintegrative disorder (Heller syndrome), one of them have changes on brain MRI suggestive of cerebral vasculitis.

A three-year girl had Rett syndrome and her case and early treatment was published [5].
She was hypotonic, ataxic and had abnormal movements of the upper limbs. She was unable to sit alone on a chair and showed no eye contact and was not responding to her name. She didn’t have purposeful hand movement and was not able to hold things. She couldn’t be held erect in the standing position. She was not saying any word nor was babbling. The girl received two treatment courses.
The first course included intramuscular cerebrolysin 1ml daily for ten days. The second course included 10 cerebrolysin injections, 3ml every third day, and oral citicoline. After the ten-day course of cerebrolysin, she showed dramatic improvement in muscle tone and was able to sit on a chair, and she had no abnormal movements. It was also possible to hold her straight in the standing position without apparent ataxia.
After the second course of treatment she showed marked improvement with the development of purposeful movement and the ability to hold feeding bottle with assistant of the mother and feed herself. She was able to stand and step one step holding furniture. She started babbling and showed some reduction in the autistic features [5].
It was not possible to document the treatment details of all patients, however, treatment was resulted in at least some improvement in all patients after variable length of treatment. Treatment was also associated with initiation of speech and improvement of repetitive behaviors in many patients.
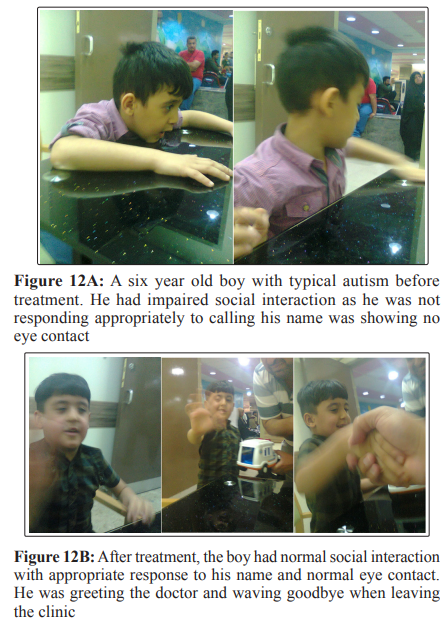
However, it was possible to document complete disappearance of the main autistic features of absence of eye contact in six patients (one boy and five girls) with typical autism, and in a boy with Asperger syndrome who was considered totally normal after treatment. Figure-12A shows a six year old boy with typical autism. He had impaired social interaction as he was not responding appropriately to calling his name was showing no eye contact.
The boy was treated for six months during which received 60 doses of Intramuscular cerebrolysin 5 ml every third day in the morning. He also received trifluoperazine 1mg at night and rochloperazine 5mg during the afternoon during the early months of treatment. He also received oral citicoline 2-3 (200-300mg) ml in the morning daily few months.
After treatment (Figure-12B), the boy had normal social interaction with appropriate response to his name and normal eye contact. He was greeting the doctor and waving goodbye when leaving the clinic.
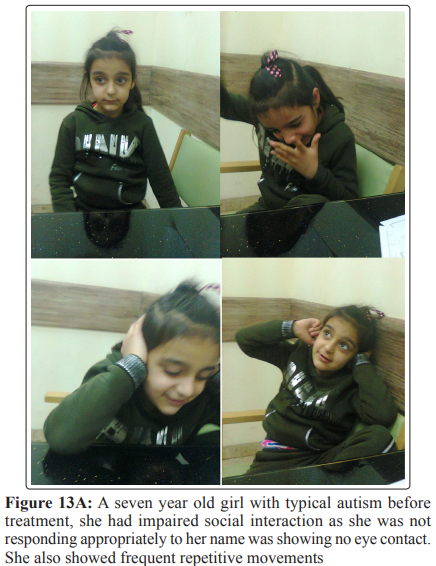
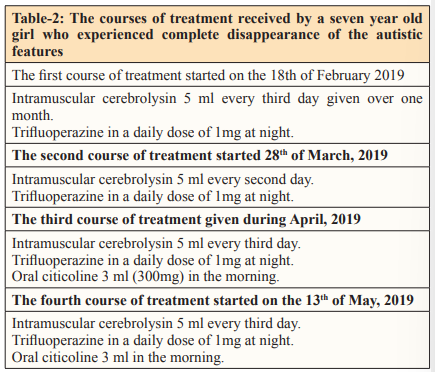
Figure-13A shows a seven year old girl with typical autism. She had impaired social interaction as she was not responding appropriately to calling her name was showing no eye contact. She also showed frequent repetitive movements. Table-2 shows the courses of treatment the girl received.
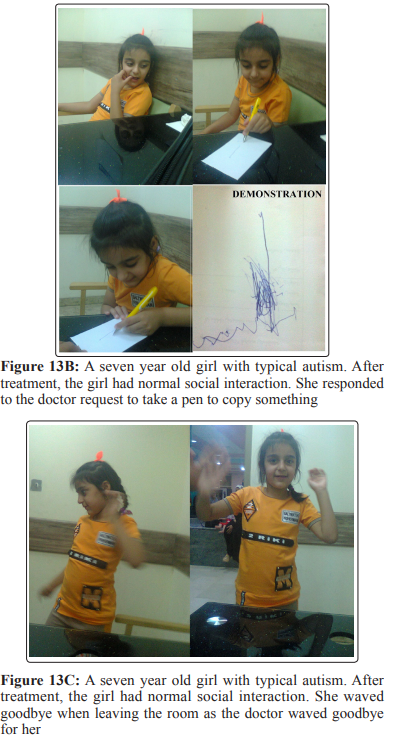
After treatment, the girl had normal social interaction with appropriate response to her name and normal eye contact. Repetitive movements disappeared. She responded to the doctor request to take a pen to copy something (Figure-13B). She waved goodbye when leaving the room as the doctor waved goodbye for her (Figure-13C).
In this series, typical autism without significant mental retardation accounted for 63%. Atypical autism (Pervasive developmental disorder not otherwise) was the second most common type of Pervasive developmental disorders accounting for about 25%. Asperger syndrome accounted for only 6% of the cases in this series.
The author would to express his gratitude for the parents of the patients who accepted publishing his photos.