Author(s): <p>Subair K, Jilu Jessy Abraham*, Nanditha Chandran, Snehal Shajith and Shana</p>
Periodontal instrumentation involves various tools essential for effective treatment of periodontal disease. Key instruments include scalers and curettes, designed for plaque and calculus removal, as well as ultrasonic devices that enhance efficiency. Hand instruments offer tactile feedback, while powered tools reduce operator fatigue and improve access to difficult areas. The choice of tools ultimately affects the quality of periodontal care and patient comfort, emphasizing the need for practitioners to be skilled in utilizing both hand and powered instruments to achieve optimal outcomes.
Periodontal instruments are intended for explicit purposes, for example, eliminating math, planning root surfaces, curetting the gingiva, and eliminating unhealthy tissue. On first examination, the range of instruments accessible for comparable purposes seem confounding. With experience, notwithstanding, clinicians select a generally little set that satisfies all necessities [1].
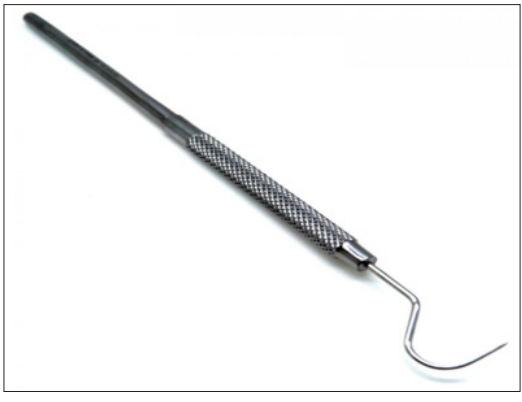
Measurements of pocket depth and pocket configuration are made with periodontal probes. To produce a pressure that indicates the approximate depth of probing, probe tips with a diameter of 0.6 mm and a force of 0.20 grammes (50 N/cm2) is exerted on the bottom of the pocket [1].

An assessment tool with a flexible wire like working end is called an explorer. The condition of the periodontal tissues, the structure of the teeth, and the texture of the tooth surfaces are assessed using equipment such as periodontal probes and explorers. When the explorer is moved across abnormalities in the tooth surface [2].
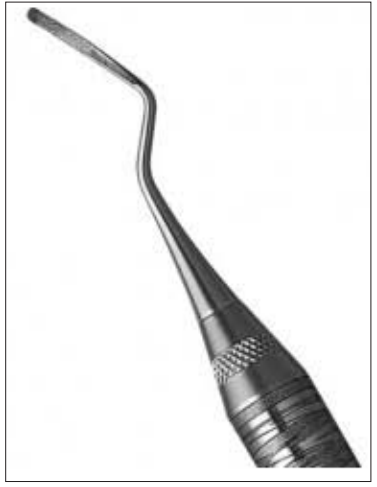
A sickle scaler is a dental tool utilized for eliminating calculus deposits from the tooth crowns. It is important to note that sickle scalers are specifically designed for supragingival use and should never be employed on root surfaces [1].

The curette is the instrument of choice for removing deep subgingival calculus, root planning altered cementum, and removing the soft tissue lining the periodontal pocket. Each working end has a cutting edge on both sides of the blade and a rounded toe [2].
A universal curette is a dental tool utilized for the elimination of small to medium-sized calculus deposits from both the crowns and roots of the teeth. Typically, this instrument is designed with two working ends that are mirror images of each other [1].

Gracey curettes are specialized instruments tailored for specific anatomical areas of the dentition. These tools, along with their variations, are highly effective for subgingival scaling and root planing due to their unique design and angulation [1].

Hoe Scalers are utilized to scale ledges or rings of calculus. The blade has a 99-degree angle bend, and the cutting edge is created by the meeting point of the flattened terminal surface and the inner aspect of the blade. The cutting edge is beveled at a 45-degree angle. The blade is slightly curved to ensure contact at two points on a convex surface. The back of the blade is rounded, and its thickness has been minimized to allow access to the roots without any hindrance from surrounding tissues [2].

The Schwartz perioretrievers are a pair of highly magnetic, double- ended tools used to retrieve damaged instruments. tips from the periodontal pocket [2].

Usually employed in the anterior region of the mouth, the chisel scaler is made for the proximal surfaces of teeth that are too tightly spaced to allow the use of other scalers. The instrument has two ends, one with a curved shank and the other straight. The blades have a 45-degree beveled straight cutting edge with a minor bend [1].

The Quétin furcation curettes are essentially hoes that fit into the furcation’s floor or roof and have a shallow, half-moon radius. Additionally, the tip’s curvature fits into the developmental depressions on the inside of the roots. There are two widths for the tips, and the shanks are somewhat bent for easier access (With a 0.9-mm blade width, the BL1 (buccal-lingual) and MD1 (mesial-distal) instruments are tiny and delicate. With a 1.3-mm blade width, the BL2 and MD2 instruments are bigger and more expansive. Even the mini-bladed curettes are frequently too big to reach some recessed sections of the furcation, and these tools remove burnished calculus from those locations [1].
Special tools called diamond-coated files are used to polish root surfaces [2].

Plaque, scaling, curing, and stain removal are all possible with ultrasonic devices 39, 40, 8, 126. Magneto strictive and piezoelectric ultrasonic units are the two varieties. In both cases, oscillations in the handpiece’s materials are caused by alternating electrical current, which vibrates the scaler tip. These ultrasonic vibrations at the tip of the instruments of both types vary from 20,000 to 45,000 cycles per second (ps; also known as Hertz [Hz]), depending on the manufacturer [1].
The elliptic vibration pattern of the tip in magneto strictive units indicates that all sides of the tip are active and will function when the unit is adjusted to the tooth The linear, or back-and-forth, vibration pattern of the tip in piezoelectric devices indicates that its two sides are the most active. A handpiece that connects to a compressed air line and uses a range of tips with certain designs makes up a sonic unit. Compared to ultrasonic units, the sonic tip’s vibrations range from 2000 to 6500 ps, which offers less power for calculus removal [2].
In order to diagnose and treat periodontal disease sub gingivally, a dental endoscope was recently launched. The Perioscopy system (Dental View, Irvine, CA) is made up of a sterile, disposable sheath that is placed over a reusable fiber optic endoscope with a diameter of 0.99 mm [2].

The motor-driven diamond files of the EVA prophylaxis instrument are perhaps the most effective and least traumatic tools for reducing overhanging of over contoured proximal alloy and resin restorations. These symmetric pairs of files are fashioned of aluminium in the form of a wedge that protrudes from a shaft; the wedge has a smooth surface on one side and a diamond coating on the other. The files can be installed on a specialized dental handpiece attachment that produces variable-frequency reciprocating strokes [1].

Rubber cups are made composed of a hollow interior and a rubber exterior that may or may not be webbed They have a unique prophylactic aspect when utilized in the handpiece. After every patient use, the handpiece, prophylactic angle, and rubber cup need to be sanitized; alternatively, a disposable plastic prophylactic angle and rubber cup can be used, then thrown away. It is best to use a fluoride-containing cleaning and polishing paste that is kept moist to reduce heat generated by friction while the cup rotates. Polishing pastes come in small, handy, single-use packages and are available in fine, medium, or coarse grits. The thin layer of cementum in the cervical area could be removed by vigorously using any kind of abrasive on the rubber cup [1].

There are wheel and cup-shaped bristle brushes. Using polishing paste, the brush is applied at the prophylactic angle. The brush should only be used on the crown due to its firm bristles in order to prevent damaging the gingiva and cementum [2].


For polishing proximal surfaces that are in reach of other polishing tools, dental tape combined with polishing paste is utilized. The tape is activated with a firm labiolingual gnat while it is passed inter proximally and maintained at a straight angle to the tooth’s long axis [2].
Early in the 1980s, a specifically made handpiece was produced that could apply an air-powered slurry of warm water and sodium bicarbonate for polishing. The Prophy-fet is an extremely useful tool for removing soft deposits and extrinsic stains. Significant tooth material loss is possible, according to research on the abrasive effect of sodium bicarbonate-based air-powder polishing machines on cementum and dentin. The air-powder polishing tool is not recommended for use in patients with hemodialysis or a history of respiratory conditions [2].
