Author(s): Yamina Elelmi*, Fatma Masmoudi, Ahlem Baaziz, Fethi Maatouk, Hichem Ghédira
Supernumerary teeth are those which are additional or in excess of the normal number. They can be present anywhere in the dental arch with predilection for the premaxilla. They can cause many complications, the most common being the delayed eruption of permanent teeth. Early diagnosis and management can minimize the potential complications caused by supernumerary teeth and the extent of surgery and orthodontic treatment.
Aim: This case report highlights the problem of delayed eruption of permanent maxillary left central incisor in a 9-year-old boy due to a supernumerary tooth. After surgical removal and 18 months of follow up, the left permanent central incisor erupted.
Several causes of delayed eruption of permanent maxillary incisors have been reported in the literature such as supernumerary teeth, tooth agenesis, tooth malformation or dilacerations, cysts or other pathological obstructions in the eruptive path, ankylosed primary teeth, lack of space or in association with certain syndromes [1, 2].
Supernumerary teeth and odontomas have been cited as the most common causes: 56-60% of supernumerary teeth cause impaction of permanent incisors due to a direct obstruction for the eruption [2, 3]. Supernumerary teeth are defined as an excess in the number of teeth present in primary or permanent dentition [5]. They are more prevalent in the permanent dentition with reports of between 1 and 3% of the general population affected [6].
Approximately, 90% of supernumerary teeth are found in the maxilla [5]. Autosomal recessive transmission pattern, or association with the X chromosom have been reported [7, 8]. The etiology of supernumerary teeth remains unknown and several theories have been suggested concerning the cause of this dental anomaly, such as the phylogenetic theory, the dichotomy theory, a hyperactive dental lamina and a combination of genetic and environmental factors [9, 10, 5, 11].
This paper reports the diagnosis and the mangement of a case which had a delayed eruption of the left permanent maxillary central incisor associated with a supernumerary tooth that was diagnosed as a mesiodens.
A 9-year-old boy consulted the Department of Pediatric Dentistry, at the Faculty of Dental Medicine of Monastir (Tunisia), with the chief complaint of unerupted left permanent maxillary central incisor. His medical history was unremarkable and there was no family history of supernumerary teeth or congenitally missing teeth. Intraoral examination showed a mixed dentition, the presence of the right maxillary permanent central incisor and the absence of the left maxillary permanent central incisor (figure1).

Figure1: Intraoral examination showing the absence of the left maxillary central incisor
Radiographic examination which was done by using ,retroalveolar radiograph and panoramic radigraph showed unerupted left maxillary permanent central incisor with immature root and a supernumerary tooth blocking its eruption. No pathosis was seen with the retained tooth, and no radicular changes were noted (figure2).
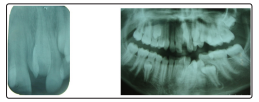
Figure 2: Radiographic examination showing supernumerary tooth blocking the eruption of the left maxillary permanent central incisor
Based on clincal and radiographic examination the extra tooth was diagnosed as a mesiodens. The treatment plan was the surgical removal of the supernumerary tooth under local anaesthesia. When the buccal flap was raised the retained permanent left central incisor and the supernumerary tooth ,were visible
The mesiodens was extracted(figure3), the flap was sutured and hemostasis was achieved.

Figure 3: Mesiodens after removal
After 18 months of clinical and radiological monitoring, the incisor erupted(Figure 4).

Figure 4: Clinical radiograph showing erupted left permanent central maxillary incisor
The patient was referred to the orthodontist to correct the alignement.
Supernumerary teeth can be classified according to their location in the dental arch as mesiodens, paramolar and distomolar or according to their morphology as conical, tuberculate, supplemental and odontome [12]. Mesiodens is the supernumerary tooth found in between the midlines of maxillary central teeth [13, 14]. In the literature, the prevalence of mesiodens were reported between 0.1-1.9% [5, 15, 16].
Supernumerary teeth frequently interfer with the eruption and alignment of the maxillary incisors, and may cause some complications such as failure of eruption, displacement, crowding, diastemas, development of odontogenic cyst, and resorption of neighboring teeth [17, 18].
They can delay or prevent eruption of central incisors in 26 to 52% of cases; cause ectopic eruption, displacement or rotation of a central incisor in 28 to 63% of cases; and labially displace incisors in 82% of cases [5, 19].
Supernumerary teeth can appear in any region of the jaws; however, they most commonly involve the premaxilla, which has also been identified as the predominant location as 80% of mesiodens were found in the maxilla [20, 17].
According to literature 75% of supenumerary teeth are asymptomatic and most cases are diagnosed by during routine radiographic inspection prior to the commencement of dental treatment [21, 22].
Maxillary occlusal radiography is highly recommended for all children with dental disturbances in the premaxilla [14]. Further more Cone Beam Computerized Tomography (CBCT) has represented an important new development in dento-maxillofacial radiology, and it has also precipitated a shift from two-dimensional to three-dimensional data acquisition, image reconstruction, and visualization .It helps in identifying the exact position of the surnumerary tooth and the amount of bone overlying so that a proper planning of the surgical procedure can be carried out [23].
Once a supernumerary tooth has been diagnosed, the clinician must decide on treatment to minimize further sequel. Different treatment modalities have been described in literature, it is partly dependent upon the position and clinical manifestation of the supernumerary tooth. Thus, making an early diagnosis is very important, in order to decide from among extraction, extraction followed by orthodontic treatment, or simply monitorization or control of the supernumerary teeth.
Surgical management in turn, ranges from removal of the supernumerary teeth, to removal of the latter, followed by orthodontic treatment which aims to ensure a correct occlusion. . In very young children the surgical removal needs more attention because of the close proximity of the developing permanent tooth. Any trauma to the developing young permanent tooth will lead to arrest in root development [24].
Timing of surgical removal of supernumerary teeth is very imporatnt, Hogstrom and Andersson suggested that early interventions are preferable to take advantage of the spontaneous eruption potential of the permanent incisors and to prevent anterior space loss and midline deviation. Extraction of supernumerary tooth at a time appropriate for promoting self-eruption in the early mixed dentition may result in better alignment of the teeth and may minimize the need for orthodontic treatment [25].
Close monitoring of the dentition is required after the extraction of a supernumerary tooth. In 75% of cases, the incisor erupts spontaneously once the supernumerary tooth has been removed [4, 26]. Di Biase and Leyland et al reported that most teeth experiencing delayed eruption will spontaneously erupt within 18 months of supernumerary removal alone [26]. Mason et al observed that more immature teeth erupted spontaneously after removal of the supernumerary compared with mature teeth [27].
In the case presented, the permanent left central incisor erupted after 18 months of clinical and radiological monotoring. The need for an orthodontic treatment to correct the alignment was explained for the patient.
When the incisors do not erupt at the expected time, it is crucial for the clinician to determine the exact etiology and formulate an appropriate treatment plan. Early diagnosis prevent complications associated with supenumerary teeth, and it is based essentially on clinical and radiographics examination.
The use of CBCT should be considered a routine diagnostic aid in cases where the treatment of supernumerary teeth is being considered, because it gives highly detailed three-dimension information.