Author(s): Mahamed Abib*, Abdinasir Abdilahi and Alimaalin Issack
Introduction: The term sexually transmitted infections (STIs) refers to a variety of clinical syndromes caused by pathogens that can be acquired and transmitted through sexual activity. STIs are caused by more than 30 different pathogens including bacteria, viruses, protozoa, fungus, and ectoparasites. Sexual transmitted diseases can lead to serious health complications and affect individual’s future reproductive plans and responsible for 17% of the total burden of disease, There is limited study done about Sexual transmitted diseases on most of regions in Ethiopia specifically in Somali region and most studies that have been done in Ethiopia were community based studies. Therefore the aim of this study was to assess magnitude and associated factors of sexual transmitted diseases among adult clients attending at public health facilities in Jigjiga town eastern Ethiopia 2021.
Methods and Materials: An institution based cross sectional study was conducted among adult clients attending Public health facilities in Jigjiga city Administrative from June 15 to july15, 2021.
Data were collected from 398 respondents by using systematic sampling technique with proportional allocation of size employed to each health facilities. Structured interview questionnaires were used to collect the data. Data were entered into the computer using Epi-data 3.1 software and exported to Statistical package for social science version 20.0 for analysis. Binary logistic regression model was carried out for analysis to identify independent predictors at p-value 0.25.
Results: The prevalence of reported ever had sexual transmitted diseases was found to be 34.5%(95%CI, 29.8-39.2) ,While assessing the independent predictors for acquiring STIs, clients who had sexual intercourse after having alcohol (AOR= 2.4; 95%CI: 1.0-6.0), clients who had multiple sexual partner in their life time (AOR=10.2; 95%CI: 3.6-28.3), as well as condom utilization was significantly associated with STD (AOR=0.064 95% CI; 0.023-0.17).
Conclusion: This study shows high prevalence of STDs among respondents. Risky of sexual behaviors like having multiple sexual partners, sexual intercourse after having alcohol; multiple sexual partners and condom utilization during intercourse were significantly associated with STDs. As a result, every STDs consultation should include preventive education, such as reducing the number of sexual partners to reduce the risk of STD.
Sexual transmitted disease refers Infections that can be transmitted from infected person to an infected person through sexual contact, Sexual contact includes: vaginal, anal or oral sexual intercourse; kissing; oral-genital contact; and the use of sexual “toys” such as vibrators. The term sexually transmitted infection applies to more than 20 different infections. It is estimated that more than 340 million new cases of curable sexually transmitted diseases (STDs) occur every year throughout the world among adults aged 15-49 years, with the second largest proportion in the region of sub Saharan Africa [1].
There are several counts of sexually transmissible etiologies from members of bacteria, viruses, and parasites. These are responsible for multiple sexually transmissible diseases such as gonorrhea, chlamydialin infection, syphilis, trichomoniasis, chancroid, genital herpes, human immunodeficiency virus (HIV) infection, and hepatitis B infection. Some of the above etiologies can also be transmitted vertically from mother to child during pregnancy as well as through blood products Sexually transmitted diseases (STDs) are also a significant public health problem, ranking them first among the top causes of disability-adjusted-life-years (DALYs) lost in urban populations in the developing world [2].
study was carried out among 65 married women of reproductive age group, the prevalence of STI was found to be 49% Parol PHC in India [3].
The World Health Organization estimated that each year more than 340 million new curable STIs occur in reproductive-aged men and women; this excludes the estimated 33 million new cases of HIV as well as estimated 100 million plus infections caused by other viral STDs each year [4].
The prevalence of STIs tends to be higher in urban residents, in unmarried individuals, and in young adults. STDs tend to occur at a younger age in females than in males, which may be explained by differences in patterns of sexual activity and in the relative rates of transmission from one sex to the other [5]. The sequelae of STDs are more serious in women because of the risk for ascending infections leading to pelvic inflammatory disease (PID), infertility, ectopic pregnancy and Increased risk of cancer of the genital tract and causes HIV [6].
However there is little information on the incidence and prevalence of STIs in Ethiopia. There are many reasons for this, but the major contributing factor is that most people with STIs do not seek treatment at public health facilities as they will have minor or no symptoms, they usually tend to take self-prescribed drugs or go to private pharmacies to buy treatment without consulting trained health workers. This study will provide prevalence and associated factors of STDs among adult clients attending jigjiga town public health facilities.
An institution based cross sectional study was conducted among adult clients attending Public health facilities in Jigjiga city Administrative from June 15 to july15, 2021.
Jigjiga is the capital city of Somali regional state located in 626 km east from Addis Ababa, Jigjiga city administration has an estimated total population of 257,613 and with 30 Keble’s of which 20 are urban & 10 are rural with (smallest administration units) constituting 17,001 households. Majority of people are Somali ethnic (97%) & Muslim in religion (98%). People of Jigjiga city are mostly agro-pastoral. The Study was conducted at selected public health facilities of jigjiga town. Jigjiga town has 1 referral hospital, 1 regional hospital and, 14 health posts, 5 public health clinics and 4 functional health centers are providing delivery services.
Data was collected by interview structured and pre-tested questionnaire first prepared in English and translated to local languages Somali for better understanding by the data collectors and respondents. The questioner was then back translated to English to check for its consistency. The questioner was developed by the principle investigator after reviewing WHO, EDHS and different literatures with modification based on research objectives. The data were collected, two-degree male nurse, two female diploma midwife and two male public health officer degree supervisors.
Sample Size Determination: Sample size was determined by using a single population proportion formula using the following assumptions: prevalence rate of abnormal Vaginal discharge (the highest of four syndromes) 38 % [7].with 5% marginal error and 95% confidence interval of certainty (alpha = 0.05). Based on this assumption, a total of 362 samples plus 10% non-response rate was included in the study. Total sample size=398 [8].
Based on monthly client flow to each adult client seeking health services in the town, systematic sampling technique was employed to select proportionate sample from each health facilities in jigjiga town and was taken based on number of adult clients, for the Last Month(march) adult clients seeking health service flow counted retrospectively to assign the required sample proportion to each health facilities and Systematic random sampling technique was used to select the respondent for interview.
A total number of 6215 of adult clients seeking health services was attended for the last month(march) for the both five public health facilities in jigjiga town, then the sample fraction of K value was obtained by dividing total population with a number of sample size, therefore the K value for each health facilities was calculated as follows JJU referral hospital K=N/n=2036/398=5 Karamara general hospital K=N/n=1750/398=4, Ablele health center K=N/ n=953/398=2, Ayardaga health center K=N/n=806/398=2 and Hanti-shacab health center K=N/n=670/398=2.
Multiple sexual partners: More than one sexual partner (57).
Consistently and Correctly Condom use: Use of a new condom for every act of vaginal sex throughout the entire sex act (from start to finish) (58).
STI: A client has said to be STI he/she fulfills one of the following
syndromes:-Urethral discharge,
Genital ulcer, Vaginal discharge, Low abdominal pain in women, & Scrotal swelling.(59)
Adult: According to WHO standard guideline the cut of point of Adult age is between 18-59years old (10).
Unsafe Sex: A susceptible person has sex with at least one partner who has an STI, without taking measures to prevent infection (60).
Good Knowledge: An individual (respondent) who respond four and above from the given 6 knowledge measuring items classified as good knowledge (59).
Poor Knowledge: An individual who respond below four items from knowledge measuring items classified as poor knowledge (59).
The returned questionnaires were checked for completeness, cleaned manually and entered in to Epi data version 3.1.
Statistical software and then transferred to SPSS windows version 20 for further analysis. Proportions, means, medians, frequency tables or cross-tabulations of important variables were used for data summarization and presentation. Descriptive statistics was performed and presented by text, tables and graphs. Chi-squared test was used to determine adequacy of the cells and association between independent variables and the outcome. Bivariate logistic regression was done and a variable with p-value < 0.25 was selected for next analysis and multicollinearity was checked. Then, multivariable logistic regression analysis was performed to identify factors independently associated with the outcome. Odds ratio was used as measure of strength of association and p-value less than 0.05 was used as statistical significance and multicollinearity was checked by variance inflation factor (VIF) goodness of model fit was checked by hosmerlemeshow goodness of fit model.
The questionnaire was initially prepared in English and then translated in to Somali language, proper designing was checked for any inconsistencies or distortions in the meaning of words and concepts and pre-testing of the questionnaires in the dagahbour Hospital other than the selected health facilities on 5% of participants, and training was given for the data collectors and supervisors before the actual data collection [10]. Every day after data collection, questionnaires was reviewed and checked for completeness and relevance by the supervisors and principal investigator and the necessary feedback was offered to data collectors prior to start the next morning data collection.
There was discussion with facilitators and supervisors accordingly if there is a problem encounter during data collection. Data quality was also ensured during data coding, cleaning, entry to computer and during analysis
Ethical clearance letter was obtained from Jigjiga University of, College of medicine and health sciences. Then, written consent was obtained from Somali regional health bureau, Jigjiga city administration and also heads of the hospitals and health centers was communicated through formal letter from city administration in addition to personal communication by the investigator. The objective of the study was explained to the study participants in order to obtain their verbal consent before interview. Participants were also informed that they have full right to discontinue or refuse to participate in the study. Answers to any questions were completely confidential. Respondents were informed on the nature and purpose of the study and were asked if they consent verbally. Confidentiality was reassured and participant was made aware that there would not be any adverse consequence to their refusal to participate.
Socio-Demographic Characteristics of Study Participants From the total sample of 398 included in the study, 383 were interviewed with a response rate of 96.2%. The mean age of respondents was 27.1(SD+ 4.77) whom, 127(33.2%) were male and 256(66.8%) were Females. While 253(66.1%) were Muslim in religion and catholic 57(14.9%), and significant proportion of the study participants were urban residents 248 (64.8%) concerning of marital status, 258(67.4%) were married and majority of 256 (66.8%) the study participants were Somali ethnicity and the age of study participants 273(71.3%) were between 25-31years and 204(53.3%) of them had an income level of >1500birr per month. Concerning of educational level 210(58.8%) of respondents were having diploma and above level. (Table 2)
Table 1: Socio-demographic characteristics of study participants attending at public health facilities in jigjiga town 2021
|
Sn |
Variable |
Category |
Frequency |
Percentage |
|
1 |
Residence |
Urban |
248 |
64.8% |
|
Rural |
135 |
35.2% |
||
|
2 |
Sex |
Male |
127 |
33.2% |
|
Female |
256 |
66.8% |
||
|
3 |
Age groups |
18-24 |
79 |
20.6% |
|
25-31 |
273 |
71.3% |
||
|
>31 |
31 |
8.1% |
||
|
4 |
Occupation of client |
Employed |
85 |
22.2% |
|
House wife |
192 |
50.1% |
||
|
Student |
53 |
13.8% |
||
|
Merchant |
53 |
13.8% |
||
|
5 |
Marital status |
Single |
86 |
22.5% |
|
Married |
258 |
67.4% |
||
|
Windowed |
30 |
7.8% |
||
|
Divorced |
9 |
2.3% |
||
|
6 |
Monthly income (ETB) |
<1500ETB |
179 |
46.7% |
|
>1500ETB |
204 |
53.3% |
||
|
7 |
Educational status |
Illiterate |
39 |
10.2% |
|
Read and write |
77 |
20.1% |
||
|
Primary |
42 |
11% |
||
|
Secondary |
15 |
3.9% |
||
|
Diploma and above |
210 |
54.8% |
||
|
8 |
Ethnicity |
Somali |
256 |
66.8% |
|
Amhara |
71 |
18.5% |
||
|
Oromo |
42 |
11.0% |
||
|
Others |
14 |
3.7% |
||
|
9 |
Religion |
Islam |
253 |
66.1% |
|
|
|
Orthodox |
52 |
13.6% |
|
Protestant |
7 |
1.8% |
||
|
Catholic |
57 |
14.9% |
||
|
Others |
14 |
3.7% |
Table 2: Occurrence of the different STDs syndromes among adult client attending at public health facilities in jigjiga town 2021
|
Variable |
Category |
Number (%) |
|
|
Ever had sexually transmitted diseases (n=383) |
Yes |
132 |
34.5% |
|
NO |
251 |
65.5% |
|
|
STDS during past 12months (n=132) |
Yes |
94 |
71.2% |
|
NO |
38 |
28.8% |
|
|
STDs during past 6months (n=132) |
Yes |
51 |
38.6% |
|
NO |
81 |
61.4% |
|
|
STDs syndrome by male During last 12 months (n= 45) |
Genital ulcer/sores |
|
9(20%) |
|
Urethral discharge |
25(55.6%) |
||
|
Scrotal swelling |
11(24.4%) |
||
|
STDs syndrome by Female During last 12 months (n=87) |
Vaginal discharge |
71(81.6%) |
|
|
Genital ulcer/sores |
7(8%) |
||
|
Lower abdominal pain |
9(10.4%)s |
||
Reported Prevalence of ever had STDs shows 132(34.5%), (95%CI, 29.8-39.2) in the study population. of those 94(71.2%) had STDs in the last 12 months prior to the data collection period. Among those ever had reported prevalence of STDs, female accounts major part 256 (66.8%), the most frequent chief complaints were vaginal discharge 71 (81.6%) in females, and urethral discharge 25(55.6%) in males (Table3).
|
Variable |
Category |
Frequency |
Percentage |
|
Have you ever heard of STDs |
Yes |
360 |
94% |
|
NO |
23 |
6% |
|
|
Can people protected from getting STD |
Yes |
271 |
70.8% |
|
NO |
112 |
29.2% |
|
|
Can STD transmitted from person who doesn’t show Any symptoms |
Yes |
80 |
29.9% |
|
NO |
201 |
52.2% |
|
|
I don’t know |
102 |
26.6% |
|
|
Are uncircumcised males More Risk STD than circumcised? |
Yes |
73 |
19.1% |
|
NO |
298 |
77.8% |
|
|
I don’t know |
12 |
3.12% |
|
|
is an early RX beneficial to STD |
Yes |
215 |
56.1% |
|
No |
131 |
34.2% |
|
|
I don’t know |
37 |
9.7% |
|
|
Can people who have STD develop additional Complications |
Yes |
170 |
44.4% |
|
No |
199 |
52% |
|
|
I don’t know |
14 |
3.7% |
The study has assessed also the level of knowledge of study participants about STDs, out of 383 were asked six knowledge related questions to assess about their knowledge of STDs, the overall 276(72%) had good knowledge about STDs and the rest had poor knowledge about STDs 107(28%) and the scores for each of the knowledge questions are described in the table below Table 4.
|
Reasons |
Frequency |
Percent |
|
Condom not available |
38 |
9.9% |
|
I Dislike condom |
245 |
64% |
|
My Partner refuse condom |
38 |
10% |
|
Trust on my partner |
7 |
1.8% |
|
Condoms are expensive |
33 |
8.6% |
|
Others |
22 |
5.7% |
Most of the participants mentioned that they have got the information related to STDs from the health institutions 314(82%), media 28(7.3%) followed by friends and magazines (figure 3).
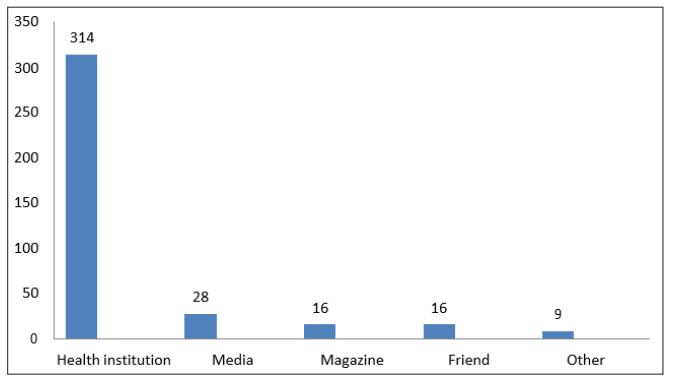
Figure 1: Source of information gained by the participants attending at public health facilities in jigjiga town Somali region eastern Ethiopia 2021.
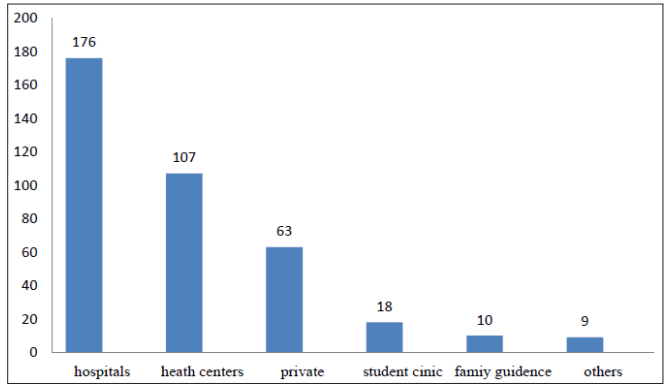
Figure 2: institutions for medical consultation of STD Among adult clients attending at public health facilities in jigjiga town Somali region eastern Ethiopia 2021
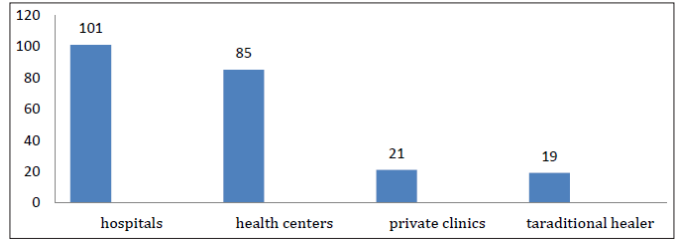
Figure 3: place of treatment seeking behavior for adult clients attending at public health facilities in jigjiga town Somali region eastern Ethiopia 2021.
Among the reported, Participants for medical consultations favored the hospitals are the highest 176(46%) clients, followed by health centers 107(27.9%) clients, and private clinics 63(16.4%) and the rest ones are students’ clinics 18(7%), family guidance association 10(2.6%), others 9(2.3%) (Figure 4).
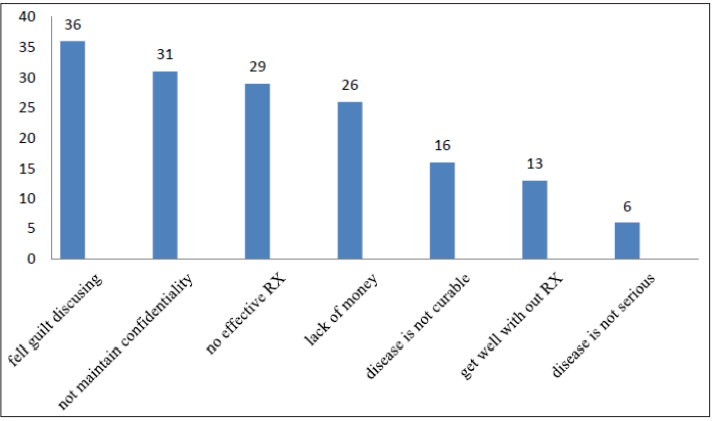
Figure 4: Reasons for delayed treatment of STD among adult clients attending at public health facilities in jigjig town, Somali region, eastern, Ethiopia, 2021
Sexual Behaviores
Among respondents, more females (69%) had reported to ever had sexual experience than males (31%) and 240(73.8%) adult clients had history of sexual practice in the last 12 months. Though 251(62.8%) of study subjects reported ever use of condom, consistent use of condom was reported only by 26(8%) and 37(11.3%) had used condom during last 12months while 288(88.6%) of them had not used. Also 61(15.9%) had history of sexual practice with commercial sex workers in the last 12 months. Among those who had sexual partner 266(69.5%) reported to have multiple sexual partners in their life, while also assessing their recent sexual practice, 32(8.4%) reported to have multiple sexual partners in the last 12 months. And From the total who reported to have sexual intercourse after taking alcohol is 69(18%) and 28(8.6%) of them used condom most of time and about 208(64%) not used condom. Respondents reported several reasons that affect them to not use condom consistently. Among those reasons are partners refuse condoms10%, trust on my partner1.8%, and condom are expensive 8.6%, dislike of condom 64% ,condom not available 9.9% and others 5.7% (table 7).
|
Variables |
Category |
Number (%) |
|
Sexual experience(n=383) |
Yes |
325(85.9%) |
|
No |
58(15.1%) |
|
|
The last 12 months history of sexual practice (n=325) |
Yes |
240 (73.8%) |
|
No |
85(26.2%) |
|
|
Ever used condom in their life time (n=325) |
Yes |
251(62.8%) |
|
No |
74(37.2%) |
|
|
Condom use in the last 12 months (n=325) |
Yes |
37(11.3%) |
|
No |
288(88.6%) |
|
|
Frequency of condom use (n=325) |
Sometimes |
63(19.3%) |
|
Most of the time |
28(8.6%) |
|
|
Always |
26(8%) |
|
|
No |
208 (64%) |
|
|
Life time number of sexual partners (n=383) |
Only one |
117(30.5%) |
|
>=2 |
266(69.5%) |
|
|
number of sexual partners in the last 12 months (n=383)
|
One |
351(91.6%) |
|
>=2 |
32(8.4%) |
|
|
Had sex with sex workers in the last 12 months(n=383) |
Yes |
61(15.9%) |
|
No |
322(84.1%) |
|
|
Sex after alcohol use in the last 12 months(n=383)
|
Yes |
69 (18%) |
|
No |
314 (82%) |
Table 6: Result of multiple logistic regression analysis of magnitude and associated factors of STDs among adult clients attending at public health facilities in jigjiga town, 2021
|
Variable |
Category |
STD STATUS |
COR (95% CI) |
P-value |
Adjusted OR (95%CI) |
P-value |
|
|
YES |
No |
||||||
|
Age In Years |
18-24yers |
41 |
38 |
1 |
|
1 |
|
|
25-31years |
65 |
208 |
3.45(2.0-5.8) |
0.00* |
1.2(0.29-5.6) |
0.73 |
|
|
>31years |
26 |
5 |
0.2(0.07-0.5) |
0.003* |
3.4(0.82-14.1) |
0.089 |
|
|
Monthly Income |
<1500ETB |
84 |
95 |
2.87(1.8-4.4) |
0.00* |
0.63(0.35-1.15) |
0.13 |
|
>1500ETB |
48 |
156 |
1 |
|
1 |
|
|
|
Life time number of sexual partner |
single |
20 |
97 |
1 |
|
1 |
|
|
Multiple |
112 |
154 |
3.52(2.0-6.0) |
0.00* |
10.2 (3.6—28.3) |
0.000* |
|
|
Had intercourse with commercial sex workers |
Yes |
39 |
22 |
4.3(2.4-7.7) |
0.000* |
1.1(0.4-2.7) |
0.77 |
|
No |
93 |
229 |
1 |
|
1 |
|
|
|
Had intercourse after having alcohol |
Yes |
45 |
24 |
4.8(2.8-8.5) |
0.000* |
2.4 (1.0- 6.0) |
0.045* |
|
No |
87 |
227 |
1 |
1 |
1 |
|
|
|
condom utilization during intercourse |
Yes |
71 |
240 |
0.053(0.027-0.10) |
0.000* |
0.064(0.023-0.17) |
0.000* |
|
No |
61 |
11 |
1 |
|
1 |
|
|
|
Number sexual partner last 12 months |
Single |
108 |
243 |
1 |
|
1 |
|
|
Multiple |
24 |
8 |
6.7(2.9-15.5) |
0.000* |
1.3(0.43-4.1) |
0.60 |
|
|
Knowledge |
Good knowledge |
72 |
204 |
1 |
|
1 |
|
|
Poor knowledge |
60 |
47 |
3.6(2.2-5.7) |
0.000* |
0.6(0.3-1.2) |
0.18 |
|
Among those who had history of STDs, 226(59%) Majority of adult clients had got treatment for the most recent syndromes that they had, for 101(44.7%) went to hospital seeking treatment of STDs Followed by health centers 85(37.6%), private clinics21 (9.2%) and traditional healer 19(8.5%) (Figure 5).
Among 157(41%) study participants had not got the treatments for the recent syndrome they had. The most important reasons for not receiving treatment by study participants were feeling guilty of telling problems to the health workers, 36(23%), 31(19.7%) not maintain confidentiality, no effective treatments 29(18.5%), lack of money 26(16.5%), thinking disease is not curable 10 16(10.2%), thinking symptoms are curable without treatment 13 (8.3%) and thinking symptoms are not serious 6(3.8%), (figure 6).
Multivariate Logistic Regression Analysis of Magnitude and Associated Factors of Stds Among Adult Clients Attending Public Health Facilities in Jigjiga Town, Somali Region, Ethiopia, July 2021. Bivariate Logistic Regression Was Done and Variables With P-Value
STDs are a major public health problem in most African countries on account of their frequency, their associated morbidity and mortality, their impact on maternal and infant health, as well as their economic costs in terms of health expenditure and lost productivity and last but not least because of their social consequences. 34.4% of participants reported to Ever had sexually transmitted to prior this study. This study, among 325 sexual experience clients, 132(34.4%) ever had STDs and 94(71.2%) had STDs in the past 12 months prior to the study period adult clients attending public health facilities in jigjiga town in the study area relatively lower when compared with the study done in Nigeria fifty five percent (55%) of the subjects harbored various agents of STDs and Up to 50% of pregnant women have been found to have vaginal discharge in sub- Saharan Africa [7]. This difference might be due to study in Nigeria included screening of all attendants by microbiologic lab investigation and included asymptomatic patients. And a study done in Zimbabwe showed that the prevalence of common sexually transmitted diseases was also 20% among women attending MCH/FP clinics [10]. Even though this disease condition poses serious burden to the public indefinitely, the healthcare system has been almost exclusively ignored for years except HIV/AIDS, particularly in resource poor countries like Ethiopia.
While assessing the sexual behavior of the participants, it was identified that 325(85.9%) (31% male and 69% female) of the attendants were sexually experienced whom 240(73.8%) were sexually experienced 12 months prior to the survey. In this study females were highly sexually experienced than males. This study was inconsistent with the study done high school students of Ethiopia, 29.1% of study population were sexually experienced of whom males accounts 66.2% and study done Agaro high school, males accounts 32.6% and the males are highly sexually experienced than females, the difference might be due to, in this study high proportion of attendants were married. Findings of this study also show that the highest rate of STDs among 25–31 years of age (71.3%) and 18-24 age group (20.6%).This result consistent with the study done in Addis Ababa, found the highest rate of STDs among 25–34 years of age and 35 to 44 age group. This implies the prevalence of STIs increased with increasing of age.
STDs affected clients in the study population, the most frequent chief complaints were vaginal discharge (81.6%), and urethral discharge (55.6%),Almost these were two times higher than the study done in Addis Ababa, the most frequent chief complaints were vaginal discharge (38.38%), combination of the sign and symptoms (28.7%) and urethral discharge (13.58%) [7]. The possible reason for this difference might be due to difference in study population, the study area of this research serves as route for commercial center for south Ethiopia, rapidly expanding town and high traffic flow that crosses over the town amongst health seeking behavior, (41%) study subjects had not got treatments for the recent syndrome they had. The most important reasons for not receiving treatment for the study subjects were feeling guilty of telling problem to a health worker, 36(23%), thinking symptom as incurable, 16(10.2%); thinking Symptom not serious 6(3.8%), thinking symptom as curable without treatment, 13(8.3%) not maintain confidentiality 31(19.7%), and Significant number of study subjects did not get treatment; this indicates. That can be taken as informative disparity provided the service is available and that they are thought to have access and affordable services.
In this study 69.5% of study subjects reported to have multiple sexual partners in their life time and of the sexually active study subjects in the previous year before the survey, 16% had reported to have sex with commercial sex workers. This is inconsistent with the study done in wolyta university, 26.3 % of study subjects reported to have multiple sexual partners in their life, and 9.8% had reported to have sex with commercial sex workers [10]. This disparity might be due to difference in study population characteristics; students may not have adequate or consistent income, and are living without consistent adult supervision.
In this study sexual intercourse after having alcohol, life time numbers of sexual partners, condom utilization during intercourse are found to have significant associated with sexually transmitted diseases. A multiple logistic regression analysis identified different independent predictors (life time number of sexual partners, condom utilization during intercourse and sexual intercourse after having alcohol) associated significantly for acquiring STDs in the study population.
Result of this study shows that clients who had sexual intercourse after alcoholic intake were about 2.4 (AOR=2.4, 95%CI, 1.0-6.0) ;( p<0.05) 2.4 Times more likely to have sexually transmitted diseases than those who had intercourse after didn’t alcoholic intake. This was nearly similar to the study done in Ethiopia on Female sex workers, alcohol use on a daily basis were found to have a 2 times increased risk of having sexually transmitted diseases (STDs) compared to the non-users of alcohol: AOR (95% CI) = 2.50 (1.35, 4.64) (60), and with study done in SNNP Ethiopia (AOR=2.05; 95% CI: 1.07, 3.94). (60). It is found that sexual intercourse after alcohol intake was one the risk factor for acquiring STDs. The possible reason might be individuals taking alcohol exposed to unprotected sex and acquire STDs.
Respondents who had multiple numbers of sexual partners were about 10.2 times (AOR=10.2, 95%CI; 3.6-28.3). ;( p<0.05) more likely to have sexually transmitted diseases than those who had single sexual partner. The total lifetime number of sexual partners was significantly associated with contracting STDs. This study finding is consistent with study done in Benin City, Nigeria; AOR 95 % CI 2.9(1.92, 4.97) which shows increasing sexual partners increases the risk of contracting STDs (61) Also study in Gondar town, North West Ethiopia history of multiple sexual partners (AOR= 3.0; 95% CI 1.9- 8.4) (28). Were significantly associations with sexual transmitted infection, the possible reason for this finding might be multiple sexual intercourse with different individuals increased acquiring STDs.
In this study, condom utilization during intercourse is associated acquiring STDs. The odd individuals who have condom utilization during intercourse had less likely (AOR=0.064 95%CI 0.023- 0.17) ;( p<0.05) to have STDs when we compared to those who do not utilize condom during intercourse. Among adult clients who had used condom during intercourse was 37(11.3%), which is consistent with studies done among Addis Ababa youth (16- 48%), and also inconsistent with study done among young adults in Dessie (56.8%) (50).That might be due to practice of condom utilization not consistent in general population. This implies majority of attendants are married and married individuals scare to use condom each sexual activity as well as married individuals have low perceived risk of acquiring STDs.
This study shows high proportion of syndromes of STDs (34.5%) and high percentage risky sexual behaviors. The prevalence of STDs was high among urban residents. Knowledge of STDs and treatment seeking behavior was high among adult clients attending at public health facilities in jigjiga town. Sexual behavioral Factors, including having multiple sexual partners, and sexual intercourse after having alcohol and condom utilization during intercourse were significantly associated with STDs.
The limitation of this study is social desirability bias due to highly sensitive questions related to sexuality. Recall bias and information bias may be another .Moreover, since this study was cross sectional, it may not allow for the establishment of a causal link to syndrome of STI.
The authors would like to acknowledge the study participants, data collectors, supervisors in the study area. Also, we would like to thank Jigjiga University, school of public health Department of Epidemiology. Last but least, we would like to thank jigjiga public health facilities for their provision of necessary information.
The authors were not funded for this work
Ethical clearance letter was obtained from Jigjiga University of, College of medicine and health sciences. Then, written consent was obtained from Somali regional health bureau, Jigjiga city administration and also heads of the hospitals and health centers was communicated through formal letter from city administration in addition to personal communication by the investigator. The objective of the study was explained to the study participants in order to obtain their verbal consent before interview. Participants were also informed that they have full right to discontinue or refuse to participate in the study. Answers to any questions were completely confidential. Respondents were informed on the nature and purpose of the study and were asked if they consent verbally. Confidentiality was reassured and participant was made aware that there would not be any adverse consequence to their refusal to participate.
Not applicable Conflict of interest None
The datasets used in the current study are available from the corresponding author.