Author(s): <p>Derqaoui Sabrine*, Essaoudi Mohamed Amine and Elktaibi Abderrahim</p>
A 85-year-old woman had a lightly pruritic firm plaque on the forearm for 28 years. She had no major medical trouble and she didn’t receive any medical treatment before visiting dermatology’s department. Biopsy specimen from the lesion revealed an amorphous a cellular eosinophilic deposits (black star) in the papillary dermis (Figure 1 A and B). The overlying epidermis was of normal thickness without hyperkeratosis (Figure 1 A and B). The deposits were negative for Congo red staining (Figure 1C), without typical green birefrengence on polarizing microscopy (Figure 1D). On immunohistochemistry, they stained diffusely positive with pan cytokeratin AE1/AE3 (Figure 2).
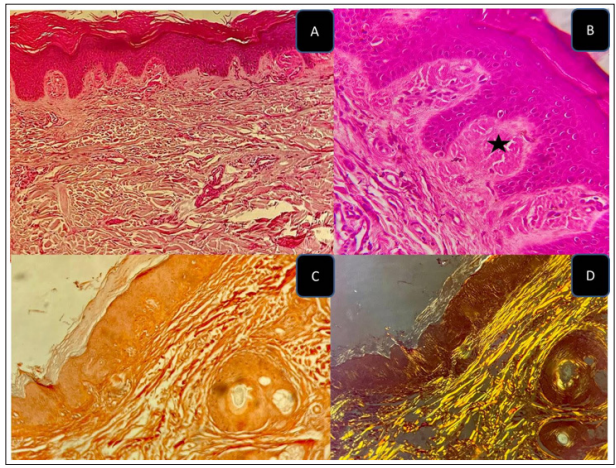
Figure 1: Amyloid Dermal Deposits : HE Stainig at Low Power (A) and High Power (B). These Deposits are Negative for Congo Red (C), Without Typical Green Birefrengence on Polarizing Microscopy (D)
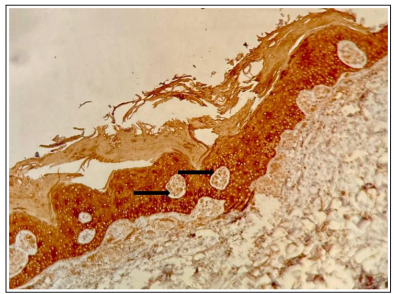
Figure 2: Immunohistochemistry : Positive Staining for pan cytoketeratin AE1/AE3
Localised cutaneous amyloidosis (LCA) is defined by the deposition of amyloid in the skin with the absence of systemic involvement LCA can be divided into: primary and secondary LCA.The latter, is observed in several inflammatory and neoplastic skin disordes such as seborrheic keratosis, Bowen’s disease and basal cell carcinoma [1,2]. Primary cutaneous amyloid is a chronic pruritic condition [1]. On histology, PCA shows amorphous eosinophilic deposits in the papillary dermis. Definite diagnosis requires special stains and sometimes immnohistochemistry Amyloid is usually positive with Congo red staining ; and shows green birefringence in polarizing micro¬scopy [3]. However, Cong red staining might be negative ; as in the present case. Immunohistochemistry for cytokeratins (high molecular weight cytokeratins and ck5/6) represents a useful diagnostic tool in LCA, because Congo red staining may not detect small deposits. In the study of et al. The authors recommend performing IHC for high molecular weight cytokeratins to exclude the diagnosis, when Congo red is negative [4]. These findings confirm the origin of amyloid : epidermal keratins due to epidermal long term damage [3].
The authors declare no competing interests
Funding Resource: Not Applicable
Informed consent was obtained