Author(s): Sawa FI, Okopi J and Chundusu CM*
The covid19 pandemic in the developing world had a far less catastrophic effect compared to that seen in the developed world. Taking a look at pre-covid19 era considering some echocardiographic parameters, left ventricular configuration was assessed.
Method and Materials: The study was a retrospective echocardiographic assessment of regular patients assessing echocardiographic evaluation without necessarily diagnosed of covid19. Kobotoolbox data collector was used for data upload and data from 2015 to 2019 were considered pre-covid19 data while those from 2020 to 2023 were considered covid19 era data and analyzed as such.
Results: Out of a total of 1,619, an average of 64% were analyzed by the collector. The two groups of population were similar considering demographic characteristic. Clinical indications pre-test had a similar distribution except in cases of dilated cardiomyopathy (p- <0.001) and stroke (p- 0.044) were the proportion were higher in pre-covd19 while chronic arrhythmias (p- 0.032) were higher during the covid19 era. The data showed a significant reduction in linear and 2D echocardiographic measurements, except for wall thickness in systole in pre-covi19 era.
Discussion: The high frequency of hypertensive heart disease during the pre-covid19 era appear to be responsible for the significant variation in the 2D and linear echocardiographic measurement.
Conclusions: This study showed that the indication for echocardiography was more diverse in the context of the COVID-19 pandemic.
The human coronavirus disease COVID-19 pandemic surprised the world, and its outcome was catastrophic, especially in the developed world [1]. The virus is highly contagious and spreads rapidly, affecting cities worldwide. The globe was totally shut down, bringing livelihood to a complete halt for months.
The WHO COVID-19 dashboard as of September 27, 2023, puts the number of confirmed COVID-19 cases at 770 million, including approximately 1 million deaths. Europe had 276 million, the Western Pacific 207 million, and the Americas had 193 million. South-East Asia, 61 million; Eastern Mediterranean, 23 million; and Africa, 9.5 million [1]. Nigeria had about 286,000 confirmed cases with a little over 3,000 deaths.
The National Centre for Disease Control (NCDC) puts Nigerian figures at 266,000 confirmed cases out of 5.7 million tested samples with approximately 3000 deaths. Lagos State had the highest number of confirmed cases and 770 deaths, FCT had 29,000 cases and 249 deaths, Rivers State had 18,000 cases and 155 deaths, and Kaduna State had 11,000 cases with 89 deaths. The Plateau State has approximately 10,000 cases with 75 deaths [2].
The Jos University Teaching Hospital, which catered for most cases in the Plateau, had an unconfirmed mortality of approximately 60 with a mortality of approximately 18. This facility has been conducting echo tests for over 20 years; however, records of this test can only be traced back approximately 12 years. The records of this echo test conducted by consultants and many resident doctors at different times in cardiology were recorded. Over 6,000 of such records were documented. The data were scrutinised and categorised into pre-COVID-19 (2012-2019) and COVID-19 (2020-2023) era data. A total of 1620 records were uploaded using the Kobotoolbox application for data entry. However, for unknown reasons, the data upload was stopped, and the proportions of the two groups were observed to be 1:1 on average. Analysis was performed to compare these two groups of records. Note that no patient was recorded as a confirmed COVID-19 patient when these tests were performed.
Hard copies of echo records were distributed to internal medicine residents for upload to the Kobotoolbox data collector, and only approximately 1620 subjects were uploaded for an unknown reason. Data from 2015 to 2019 were considered pre-covid19 data while those from 2020 to 2023 were considered covid19 era data and analyzed as such. Average values of left ventricular parameters were downloaded for analysis and categorised into pre-COVID-19 and COVID-19 era groups. More than 60% of the data results were analysed despite extensive data cleaning.
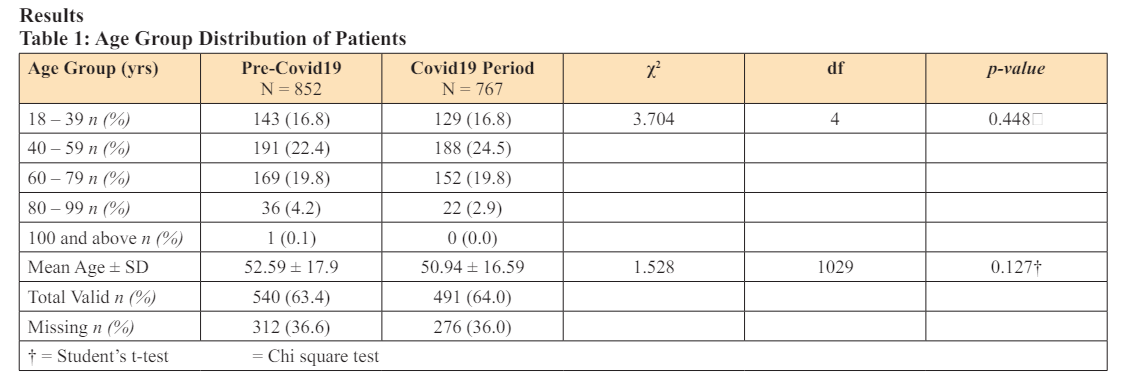
The analysis was done with IBM Statistical Package for Social Sciences Statistics (SPSS) version 27.0 software. Discrete variables were entered as mean and standard deviation for age and sex. Student’s t-test was used to assess p-values. Age groups were entered as absolute figures and proportions, and the p-value was determined using the chi-square test. Ethical clearance was obtained from the ethical committee of Jos University Teaching Hospital. There were no conflicts of interest during the compilation of these data.

Bearing in mind that the study was not conducted among confirmed COVID-19 cases, the expectation was to look at a clinical approach to the population when the COVID-19 pandemic occurred.
First, the use of a non-scientific sampling method applied during the study appeared not to have any impact on the outcome of the study because the two study groups were homogeneous. Similarly, the proportions of age groups were almost equally proportioned.
High proportions of specific clinical indications of hypertension, hypertensive heart diseases, congestive cardiac failure, and ischaemic stroke were observed and reflected similarly to studies on cardiovascular risk in many centres locally and internationally [3- 5]. This study showed that before the era of COVID-19, there were on average high indications for dilated cardiomyopathy and stroke when requesting echocardiography. Arrhythmia, on the other hand, was seen to be a more frequent indication for echocardiography with the arrival of the COVID-19 pandemic. Although arrhythmia is mostly attributed to heart-related conditions, it is also associated with anxiety, psychological states, or general illness behaviour [6-9]. We felt that this was probably more common with the emergence of COVID-19. Illness behaviour from psychological stress could also result from other clinical states undefined or captured in this study not only COVID-19.
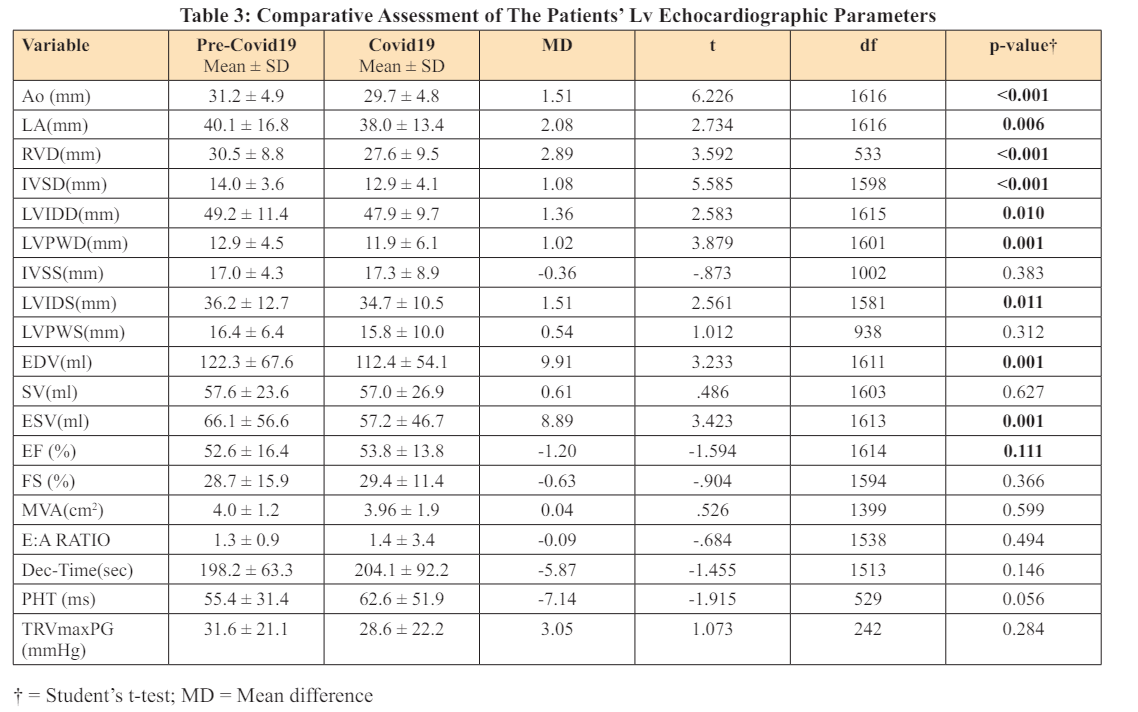
Echocardiography remains the cornerstone of all cardiovascular evaluations [10,11]. This invasive procedure is still evolving with scientific breakthroughs that give astonishing results. It is accepted worldwide for cardiovascular evaluations [11-13]. Various parameters obtained from this test categorise heart abnormalities in various terms. Systolic/diastolic abnormality or dysfunction can be assessed with linear measurement in M-mode, area and volume in 2D mode, flow Doppler, and more recently tissue Doppler and speckle tracking methods. The linear measurement and 2D records were analysed in the course of this study. [Table 3].
The data showed a significant reduction in linear and 2D measurements, except for wall thickness in systole in pre-covi19 era. Ejection fraction and fractional shortening (EF & FS) were not significantly different. This reduction in linear and 2D results was not surprising as there were more subjects with hypertension and heart diseases in the pre-COVID-19 group, which would have had a detrimental effect on cardiac function. Perhaps, the relatively high mean age in the precovid19 group partly contributed to some extent. Another reason could also be that clinicians in the precovid19 era requested echocardiography for mainly cardiovascular related diseases. Therefore, with the COVID-19 pandemic, “illdefined” clinical conditions form part of a significant indications for echocardiography. If not, one would be tempted to say that the subjects tested during the COVID-19 pandemic had better records in terms of left ventricular systolic functions of the heart.
The sampling method and the size of this retrospective study were not scientific. Approximately 40% of the subject data was lost due to data cleaning, which reduced the actual data analysed. Echocardiography was conducted over a long period of time, more than 6 years, by more than 20 different doctors, and there was a gradual improvement in data quality with time. Data were recorded using more than one machine contributing to further variations.
This study showed that the indication for echocardiography was more diverse in the context of the COVID-19 pandemic.