Author(s): Akter Hossain
Introduction: The human forearm serves an important role in upper extremity function, facilitating placement of the hand in space, thus helping to provide the upper extremity with its unique mobility Fractures involving the bones of forearm present unique problem not encountered with fractures of other long bones.
Objective: To evaluate and compare the outcomes of locking compression plate (LCP) with limited contact dynamic compression plate (LC-DCP) for the treatment of adult diaphyseal both bone forearm fractures.
Material and Methods: This study conducted in the Department of orthopedics, Mymensingh Medical College Hospital, Mymensingh, Bangladesh from January 2018 to December 2020 included 20 patients with 40 fractures in each group. Patients were selected randomly to receive either LCP (20 patients, 40 fractures) or LC-DCP (20 patients, 40 fractures). Operative time, callus formation, functional outcome and complications were recorded.
Results: Mean operative time did not differ significantly in the LCP and LC-DCP group (71.25 and 75.70 minutes respectively) .There was some difference in callus formation and mean time to bone union between the two groups which was significant. However, overall functional outcome did not differ significantly between both the groups. One case had delayed union in the (LC-DCP) group while one patient in each group developed superficial infection.
Conclusion: In this prospective study comparing LCP with LC-DCP, the outcomes were equal in terms of final functional outcomes and mean operating time but LCP showed slight advantage in terms of callus formation and mean time to bone union.
The human forearm serves an important role in upper extremity function, facilitating placement of the hand in space, thus helping to provide the upper extremity with its unique mobility. The presence of the proximal and distal radio ulnar joints allows pronation and supination and such movements are important to all of us in the usual activities of daily living. Moreover, the forearm serves as the origin for muscles inserting on the hand. Therefore, fracture involving the bones of the forearm present unique problems not encountered with fractured of other long bones and may significantly affect the function of the upper limb [1]. Since radius and ulna articulate with one another at both distal and proximal end, the integrity of these joints is a further essential ingrediant in achieving excellant long term result after injury. Malunion and non-union are more frequent because of the difficulty in reducing and maintaining the reduction of two parallel bones in the presence of pronating and supinating muscles that have angulating and rotational influences. Because of these factors, open reduction and internal fixation for diaphyseal fracture in the adults are generally accepted as the best method of treatment, even though closed reduction may be achieved [2]. Treatment by closed reduction and cast immobilization results in a poor functional outcome with unsatisfactory results reported in up to 92% of cases, usually caused by malunion, non-union or syntosis [3-5]. Various types of plates are available for open reduction and internal fixation using plate and screws. The 3.5 mm LC-DCP ( Limited contact dynamic compression plate) remains the gold standard for internal fixation of forearm fractures [3]. The LC-DCP has groove within the undersurface (leads to an improvement in the blood supply to the underlying plate bone segment) allows for a small amount of callus formation as well as even distribution of stiffness along the plate, undercut plate holes allow extended tilting of plate screws, uniformly spaced as well as symmetrical plate holes and has an optimal screw effect [6,7]. The LCDCP was claimed to reduce the bone plate contact by approximately 50% [8,9]. The newly developed Locking compression plate (LCP) consists of self-compression plate and screw system where the screw are locked in the plate. This locking minimizes the compressive forces exerted on the bone by the plate. This means that the plate does not need to touch bone surface at all. LCP can be used in forearm fractures in the conventional plating technique (compression method - principle of absolute stability) for simple transverse or oblique fracture with low soft tissue compromise or in the bridging technique (internal fixator method principle of relative stability) for comminuted fractures if required; or in the combination technique (compression and bridge technique) in special situation (e.g. segmental fracture with two different fracture pattern one simple and one multifragmentory. It is unclear whether a bridging technique or a combination of compression and bridging is beneficial for simple transverse or oblique forearm fractures [10].(10) Although the LCP represents the latest development in plate development, its usage in fractures with simple configuration and in superiority over conventional plating system (LC-DCP) is yet to be proved [11]. The aim & objects of this prospective comparative study was to analyze and compare the outcomes of using the Locking compression plate (LCP) and Limited contact dynamic compression plate (LC-DCP) for internal fixation in adult diaphyseal both bone forearm fractures in terms of fracture union, range of motion, and functional outcome.
This study conducted in the Department of orthopedics, Mymensingh Medical College Hospital, Mymensingh, Bangladesh from January 2018 to December 2020 included 20 patients with 40 fractures in each group. Patients were selected randomly to receive either LCP (20 patients, 40 fractures) or LC-DCP (20 patients, 40 fractures). We conducted a prospective study on patients >18 years with closed or open type I and II, simple transverse or short oblique fractures of shaft of both bones of forearm (<21 days old). 20 patients with 40 fractures of forearm were treated with open reduction and internal fixation with 3.5 mm stainless steel LCP and another 20 patients with 40 fractures of both bones of forearm were treated with open reduction and internal fixation with 3.5 mm stainless steel LCDCP. On admission of patient, a thorough clinical examination was done including systemic examination to rule out any associated any injury. Antero-posterior and lateral radiographs of affected forearm including elbow & wrist joint were done. The radius was exposed through the Anterior Henry approach and the plate applied to volar surface, when the fracture was on the lower two-third or through the dorsal Thompson approach and the plate placed on the dorsal plate when the fracture was on upper third. The ulna was exposed through the postero medial subcutaneous surface and the plate was applied on the posterior surface since it is the tension side of ulna. Radius was fixed first followed by ulna (fig-1 and fig-2). The patient were called for checkup first on 14th post- operative day and then on completion of 4 weeks and later after every 2 weeks .The Results were evaluated on the basis of fracture union, range of motion and complication
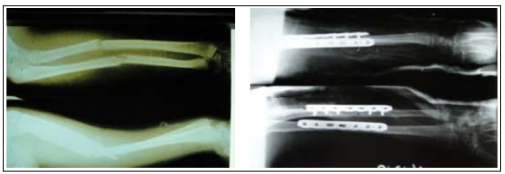
Figure 1: Showing pre and post-operative photograph in LCP Fixation group

Figure 2: Showing pre and post-operative radiograph in LCDCP group Fixation
Criteria for Union bone union are defined as obliteration of fracture gap or the presence of bridging periosteal callus in radiograph. Callus formation in the fractures is classified as: none, minimal, moderate and abundant. The criteria of Leung F et al [12]. were used in determining status of union. Union: fractures which healed in less than six months.
Delayed union: those which required more than six months to unit but without any additional operative procedures. Non-Union: those which failed to unite without another operative procedure.
Criteria for functional results: The Criteria of Anderson et al [11]. were used in grading the functional outcome, which is as follows (Table-1):
| Results | Union | Flexion and extension at Elbow joint | Supination and pronation |
|---|---|---|---|
| Excellent | Present | < 100 Loss | < 25% loss |
| Satisfactory | Present | < 200 loss | < 50% loss |
| Unsatisfactory | Present | > 200 loss | > 50% loss |
| Failure | Non - union or unresolved chronic osteomyelitis | ||
Data Analysis: Subjective assessment was done using the Quick DASH score. Statistical analysis was made using the software SPSS 20. Difference was considered significant when the p value was <0.05.
There were 13 males and 7 females in LCP group and 11 males and 9 females in LCDCP group. Male outnumbered females in our study in both groups. The mean age of patient in LCP group was 32.55 years and in LCDCP group it was 33.40 years. There were 13 fracture of the both bone of forearm on left side and 7 on right side in LCP group. In LCDCP group, 11 fractures of both bones of forearm on left side and 9 on right side. Thus there was predominant involvement of the forearm of the left side and a consequent higher rate of involvement of the non- dominant forearm in both groups in our study. The causes of injury was road traffic accidents in 10 cases, fall from height in 10 cases, assault in 3 cases and sport injury in 1 case in LCP group. In LCDCP group, RTA was causative factor in 8 cases, fall from height in 7 cases, sport injury 3 cases and assault in 2 cases. RTA was found to be most common mode of injury in both groups followed by fall. There were 12 cases of both bones of forearm fractures involving middle third region, 5 cases involving lower third and 2 cases in upper third in LCP groups. In LCDCP group, 11 cases involved middle third of forearm; lower third was involved in 7 cases and upper third in 2 cases. In our study, middle third region was most commonly involved in fracture of both bones of forearm in adult. The average age of fractures at surgery in LCP group was 7.55 days and in LCDCP group it was 7.30 days. Standard AO principles were followed and the surgeries were done according to the AO accepted standard procedures. Bone graft was not used in any of our patient in any groups. Average operating time in LCP group was 71.25 minutes and in LCDCP group it was 75.50 minutes. In our study, abundant callus formation was present in 4 cases, moderate in 6 cases and minimum in 3 cases and no callus formation was there in 7 cases in LCP group while in LCDCP group, abundant callus formation was seen in 2 cases, moderate in 3 cases and minimum in 2 cases and no callus formation was there in 13 cases. Thus callus formation was seen in sixty five percent in LCP group and thirty five percent in LCDCP group. (Fig 3) The union rate was 100% in both groups, with one delayed union in LDCDP group. The Mean time to union was 13.90 weeks in LCP group and 16.80 weeks in LCDCP group. (Fig 4).
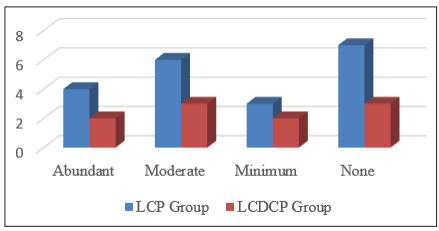
Figure 3: Showing amount of callus in both group
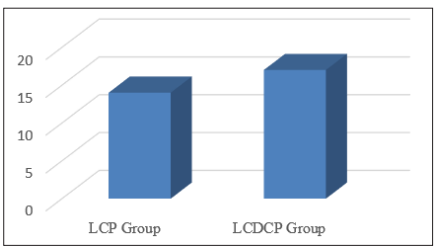
Figure 4: Showing duration of fracture union in both groups
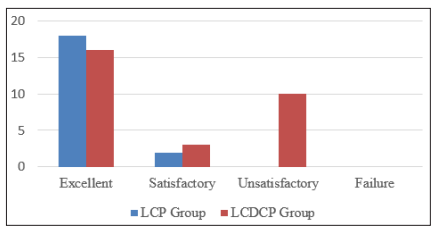
Figure 5: Showing functional outcome in LCP and LCDCP group
We had excellent functional outcome in 18 patients (90%), satisfactory in 2 cases (10%) in LCP group. In LCDCP group, excellent functional outcome was there in 16 cases (85%), satisfactory in 3 patients (15%) and unsatisfactory in 1 case (5%) with no failure in both groups. (Fig 5). In both groups, one patient each developed superficial infection. Infection was controlled with appropriate antibiotics after culture and sensitivity. In LCP group, one patient developed transient neuropraxia of the radial nerve. He had wrist drop and it was most likely a high radial nerve neuropraxia, probably from external compression. He was managed conservatively with supportive measures in the form of cock-up splint, multivitamins and active physiotherapy. He had a remarkable improvement and had full recovery by the end of 3 months. One patient in LCDCP group had delayed union but which become eventually united without any operative intervention. The quick Dash questionnaire was used to assess the outcome subjectively. The raw score ranged from 0 to 24.22 in LCP group and 0 to 38.40 in LCDCP group. Overall, the patients were satisfied with the outcome in both groups. In our study, we struck on the principle of not removing the implant for at least 18 months after plating or unless clearly indicated. Only one implant removal was done in each group and no implant related complications was observed in our study.
In our present study the average age of patient in LCP group was 32.55 years (S.D ± 11.50) with range being 18-64 years and in LC-DCP group, average age of patient was 33.40 years (S.D. ± 11.92) with range being 18-60 years. This data is similar to the finding of Saikia et al [13]. where the average ages was 29 years, Leung F et al [12]. where the mean age was 35 years and Sharma S. et al [14]. where the mean age was 34 years. Overall there were 24 males in both group comprising 60%, male to female ratio being 1.5:1. The predominance of male may be because of the fact that they are more exposed to outside environment like riding vehicle, heavy manual work, and sports in comparison to their female counterparts. The difference between the two groups was insignificant (P>0.05). This finding is similar to Saika et al [13]. where males constituted (70%) and female (30%), and Manjappa CN et al15 where 75% were males and 25% were females. There were 13 fractures (65%) on the left side and 7 fractures (35%) on the right forearm in LCP group while in LCDCP group; there were 11 fractures (55%) on the left side and 9 fractures (45%) on right forearm. The difference was insignificant (P>0.05). This data was similar to the finding of Manjappa CN et al [15]. where left forearm was involved in 12 patients (60%) and right forearm fracture was seen 8 patients (40%). Majority of patients had fractures in their non-dominant forearm as in LCP group non -dominant forearm was involved in 70% cases and in LCDCP group it was involved in 55% cases. The difference between the two group was statistically insignificant (P>0.05). This data is similar to observation made by Singh S et al [16]. That reported involvement of the non-dominance extremity in 58% of the cases. In our present study, RTA was most common cause of injury in 10 cases (50%), followed by fall from height 5 cases (25%), assault in 3 cases (15%) and sport injuries in 2 cases (10%) in LCP group. In LCDCP group, RTA accounted for 8 cases (40%), followed by fall from height in 7 cases (35%), sport injuries 3 cases (15%) and assault in 2 cases (10%). The difference between the two groups is not significant (P>0.05). This data is similar to study conducted by Singh S. et al [16]. Where RTA constituted 64% of cases and fall from height (12%). Marya KM et al [17]. Reported RTA to be responsible for 88 % of fractures of both bones of the forearm there were 12 cases (60%) of both bone of forearm fractures in middle third region. followed by 5 cases (25%) in lower third and 3 cases (15%) in upper third in LCP Group. In LCDCP group, middle third region constituted 11 cases (55%), lower third was involved in 7 cases (35%) and upper third accounted for 2 cases (10%). The difference between the two groups was not significant (P values > 0.05). This date was similar to study conducted by Marya KM et al [17]. Where middle third of the forearm bones were involved in 52 % of fractures. In Manjappa CN et al [15], 60% patients had diaphyseal fracture involving middle third region, 25 % had proximal third fracture and 15% had lower third fracture. The mean age of fracture in LCP group was 7.55 days while it was 7.30 days in LCDCP group, range being 3 to 20 days in both groups. The difference between both groups is statistically insignificant (P>0.05). 60% of patient in LCP group and 65% in LCDCP group were operated within one week of their presentation to our institution. Though there was no case of non -union, we feel that operating upon first week after the injury is technically a bit easier since the organization of the exudates and shortening of the muscle later on, may make the surgery more difficult. The operative time ranged from 65-105 minutes in LCP group with mean operative time being 71.25 minutes and Std. deviation of 11.10 while in LC-DCP group, mean operative time was 75.50 minutes, Std. deviation of 10.247 with range from 60 - 100 minutes. The difference in the duration of operation was not found to be significant to influence the outcome of the procedures. In Saikia KC et al [13], mean operating time was 93.05 minutes with range being 75- 180 minutes for LCP fixation while in LCDCP mean operating time was 81-94 minutes with range as 60-100 minutes. In LCP group, there was abundant callus formation in 4 cases (20%), moderate in 6 (30%), minimum in 3 case (15%) and no callus formation in 7(35%) while in LCDCP group abundant callus was seen in 2 cases (10%), moderate in 3 cases (15%), minimum in 2 cases (10%) and no callus was seen in 13 cases(65%). Thus, callus formation was seen in sixty five percent in LCP group and thirty five percent in LCDCP group. The difference between the two groups was statistically significant (p<0.05). Saikia et al [13]. reported that 56% of forearm in the LCP group healed with radiological evidence of callus formation of which, 17% showed abundant callus formation, 22% showed moderate callus formation, 17% showed minimal callus and the rest 44% had no callus formation while in the LC-DCP group, 83% of the forearms did not show any callus formation, 11% showed minimal Callus formation, 6% showed moderate callus while abundant callus formation was not seen. The Mean time for union for the forearms fixed with LCP was found to be 13.90 weeks (range 8 - 18 weeks) in comparison to 16.80 weeks (range 14-24 weeks) for the LCDCP group. The difference between the two groups was statistically significant (P <0.05). In the study conducted by Saikia et al [13], the Mean time for union for the forearms fixed with LCP was found to be 14.16 weeks (range 8-21 weeks) in comparison to 16.27 weeks (range 10-29 weeks) for the LCDCP group. Sharma S et al [14]. In their study of diaphyseal forearm bone fractures by locking compression plate (LCP) reported mean union time of 12.6 weeks with range being 8-24 weeks. Manjappa CN et al [15]. in their study of surgical management of forearm bone fractures in adults using limited contact Dynamic Compression plate reported average time for union as 17 weeks. Leung F et al [12]. In their study of locking compression plate in the treatment of forearm fracture reported mean union time to be 20 weeks (range 8-36 weeks). There was excellent functional outcome result in 18 patient (90%), satisfactory in 2 patients (10%) in LCP group. In LCDCP group, excellent functional outcome was seen in 16 patient (80%), satisfactory in 3 patient (15%) and unsatisfactory in 1 patient (5%). The score at the latest follow up was considered. The raw score ranged from 0 to 24.00 in LCP group and 0 to 33.40 in LC-DCP group. Saikai KC et al [13]. Observed that the raw score ranged from 0 to 22.32 in the LCP group and o to 44.44 in the LC-DCP group. In our study, the patient who had developed highest disability score or 22 was in LCDCP group. The patient was on irregular follow up visits and did not comply with the advice of physiotherapist. Overall, the patients were satisfied with the outcomes in both the groups. The difference between the two groups is statistically insignificant. (P >0.05). Saikia KC et al [13] observed excellent functional outcome in 32 patients (89%), satisfactory outcome in 3 patients (8%), and unsatisfactory outcome in 1% patient (3%) without any failure. Marya KM et al, in their study of limited contact Dynamic compression plate for adult forearm fracture reported excellent functional outcome in 88% cases, satisfactory for 7% cases, unsatisfactory in 4% cases and failure in 1%. The Quick Dash score was used to assess the outcome subjectively [17].
The results of LCP and LCDCP fixation were significant in terms of mean time to union and Callus formation between the two groups, which showed definite advantage in respect to LCP fixation for adult diaphyseal fractures of the both bones of the forearm but difference in overall functional outcome in both groups was not significant. Both groups had 100% union rate without any failure. The limitation of our study was small sample size in both groups and absence of long term follow-up. We are of opinions that open reduction and internal fixation with LCP and LCDCP provides excellent functional results in terms of union rate as well as functional outcome. A randomized control trial, preferably triple blinded or at least double blinded in nature, involving a large number of patients with long term follow up is clearly indicated to bring out significant difference between LCP and LCDCP fixation in fractures of the both bones of the forearm.