Author(s): <p>Chang Stephen Kin Yong* and R Ang</p>
Introduction: The laparoscopic approach in liver surgery has been preferred over the traditional approach in the resection of segments 2 and 3, as laparoscopic surgical technique can be standardized for easy adoption and is minimally invasive. This paper describes the laparoscopic surgical technique and recommends the patient selection criteria in the resection of segments 2, 3 and 4.
Methods: This technique involves 2 key steps – early division of the left pedicle before the division of the liver parenchyma and the placement of an instrument beneath the transection plane to simulate a ‘hanging manoeuvre’ with reduced blood loss and allows the expeditious division of the liver parenchyma. Apart from the usual contraindications to liver resections, specific contraindications to this technique include patients with aberrant biliary drainage of right liver segments into the left hepatic duct, patients with tumours abutting the hilar plate and patients with tumours located near the junction of the left hepatic vein and the vena cava.
Conclusion: The authors recommend these steps to serve as a standardized technique for laparoscopic hepatectomy of segments 2,3 and 4 in selected patients, allowing the learning curve for this technique to be markedly shortened.
The laparoscopic approach to abdominal surgery is increasingly being recognized to be the approach of choice compared to the traditional open laparotomy approach given the many benefits of minimally invasive surgery such as post-operative pain reduction, fewer wound complications and faster recovery from surgery. Similarly in liver surgery, there is increasing adoption of the laparoscopic approach [1]. Notably, laparoscopic left sectionectomy has been recommended to be the routine approach for resecting segments 2 and 3 of the liver. Herein we describe our technique and steps in performing laparoscopic hepatectomy for segments 2, 3 and 4 and recommend the patient selection criteria in adopting this approach as a routine approach [2].
The patient lies in a French position with legs straightened and apart and well strapped to allow reverse Trendelenburg position. Pneumoperitoneum pressure is kept at 12 mmHg. A camera port is placed on the umbilicus, 2 working ports on the right hypochondrium, 1 at epigastrium and 1 at the left hypochondrium (Figure 1). Instruments such as hooks, ultrasound (to assess margin), cotton tapes, goldfinger dissectors (FLEXLAP®, Advanced Endoscopy devices, Los Angeles, California, USA), forceps and linear staplers are needed for the procedure. The round ligament is first divided close to the abdominal wall and the falciform ligament is divided high against the anterior abdominal wall and continued cephalad to expose the junction of the hepatic veins draining into the inferior vena cava. The left lobe of the liver is then freed from the diaphragm by dividing the left triangular ligament (Figure 2). The hepatoduodenal structures are slung in preparation for pringle manoeuvre (Figure 3). The lesser omentum and Arantius ligament are divided (Figure 4) and the cephalad edge of the left portal pedicle is identified. Hepatotomy at segment 4 just anterior to the hilar plate and just medial to the left pedicle (Figure 5) is performed to a depth into the liver parenchymal such that the left pedicle can be encircled. The left pedicle is then encircled with cotton tape (Figure 6) with the help of a Goldfinger dissector. A linear stapler with a vascular cartridge is used to divide the left pedicle (Figure 7). A clear vascular demarcation can then be seen between the right lobe of the liver and segment 4 of the liver (Figure 8). Rubber bands (Figure 9) are now sutured to the two sides of the transection plane to aid in opening and stabilizing the liver while it is being divided using ultrasonic cavitation devices with coagulation of vessels using bipolar devices. Nearing the end of the resection, a laparoscopic instrument can be used to lift up the left lobe of the liver at the transection plane to provide a ‘hanging manoeuvre’ to allow the parenchyma division to be performed expeditiously towards the left hepatic vein (Figure 10), whereupon the left hepatic vein is encircled with a cotton tape with the help of a Goldfinger dissector in preparation to be stapled (Figure 11) (If the left hepatic vein is not easily exposed, it can be taped together with liver tissue surrounding it). Lastly, the specimen was extracted through a protective bag through an extended umbilical port incision or previous laparotomy scar or Pfannenstiel incision.
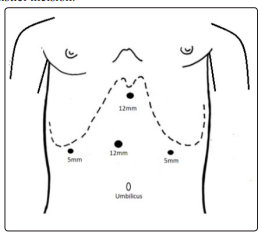
Figure 1: A camera port was placed in the umbilicus, with 2 working ports on the right hypochondrium, 1 at epigastrium and 1 at the left hypochondrium

Figure 2: The left lobe of the liver is then freed from the diaphragm by dividing the left triangular ligamen
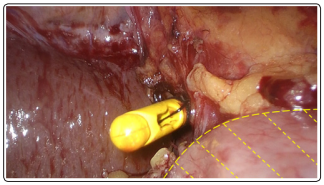
Figure 3: Hepatoduodenal structures slung in preparation for pringle manoeuvre. (The shaded yellow region is the duodenum)
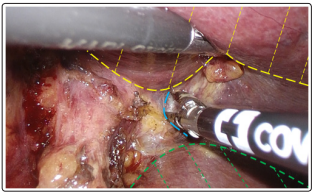
Figure 4: Division of the lesser omentum and Arantius ligament. The dotted blue line denotes the cephalad edge of the left pedicle. The shaded yellow region is the left lobe and the shaded green region is the caudate lobe
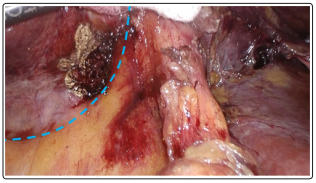
Figure 5: Hepatotomy at segment 4 just anterior to the hilar plate (the blue dotted line) and just medial to the left pedicle
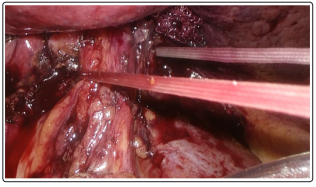
Figure 6: Left pedicle is encircled with cotton tape
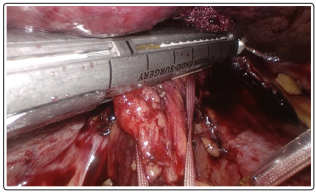
Figure 7: A linear stapler with a vascular cartridge is used to divide the left pedicle

Figure 8: Following the division of the left pedicle, a clear vascular demarcation can then be seen between the right lobe of the liver and segment 4 of the liver. (Dotted white line)
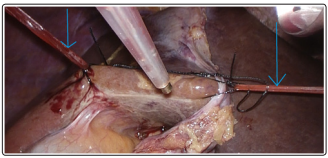
Figure 9: Rubber bands (pointed by the blue arrows) sutured to the two sides of the transection plane to aid in opening and stabilizing the liver while it is being divided.
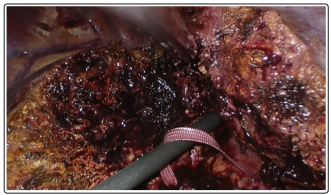
Figure 10: ‘Hanging manoeuvre’ using a straight instrument to lift the transection plane
Apart from the usual contraindications to liver resections (such as inadequate liver reserves or presence of metastases etc.), there are some specific contraindications to this technique for laparoscopic left hepatectomy.
Firstly, patients who have aberrant biliary drainage of right liver segments into the left hepatic duct will not be suitable as it will lead to persistent bile leak from the divided unconnected biliary segmental pedicle [3].
Secondly, patients with tumours abutting the hilar plate may prove to be unsuitable for this technique because the hepatotomy at segment 4 may result in inadvertent trespass into the tumor.
Finally, patients with tumours located near the junction of the left hepatic vein and the vena cava may also preclude this approach for fear of inadequacy of tumor margin when dividing the left hepatic vein using the stapler.
Laparoscopic left lateral sectionectomy has been recognised as the approach of choice2 in resection of segments 2 and 3 of the liver, as the steps in performing the surgery can be standardized and can be fairly easily adopted by new adopters of the laparoscopic approach to liver surgery. In this paper, we recommend the procedure and steps of laparoscopic resection of segments 2, 3 and 4 of the liver and believe this too can be adopted safely as the routine approach.
A key step in this approach is the early division of the left pedicle before the division of the liver parenchyma. This can be done with a small hepatotomy above the hilar plate and just medial to the left portal pedicle. No large vascular structure is present in this part of the liver and thus this can be performed with minimal blood loss.
Another useful step is the placement of an instrument beneath the transection plane along the groove between the left liver lobe and caudate lobe to simulate a ‘hanging manoeuvre’. This technique reduces the venous pressure from the vena cava and helps reduce blood loss and allow the division of the liver parenchyma expeditiously.
As the vascular aberrancy of the left lobe is rare, with the use of these standardized steps, the learning curve for this technique can be markedly shortened.
We hope this serves as a standardized technique to allow laparoscopic hepatectomy for segments 2, 3 and 4 to be adopted as a new routine approach.