Author(s): Mohammed Legas, Roza Teshome and Workinesh Sinashaw Ababe*
Maternal mortality refers to deaths with related to complications in pregnancy or childbirth or the death of the mother with in fortytwo days of after delivery. Worldwide, the maternal mortalityratio (MMR) was an estimated of 216 maternal deaths per 100 000 live births in 2015. From those developing regions account for approximately 99% and sub-Saharan Africa alone accounting for 66%, followed by Southern Asia [1].
Even if high MMR is a one of the main concern of health problem of most country in the world, different project and strategies are approved that it is reducible ;even though still the reduction is not reached the excepted level of goal (70 /100 000 live births) [1,2]. Ethiopia is also one of the sub Saharan country which have 412 maternal mortality for every 100,000 live births in 2016 [3]. The Percentage of women aged 15-49 years that were attended at least.
Most of the cause of maternal deaths are preventable and the effect of three delays, from which the major one is delay in seeking care. poor knowledge about obstetric danger sign is a major contributor for this delaines. The percentage of women age 15- 49 years that were attended at least once ANC during pregnancy by skilled health personnel (doctor, nurse, or midwife) in sub Saharan countries were low, this may be related with inadequate knowledge [4].
Every pregnant woman faces the risk of sudden unpredictable complication that could end with death or injury to the mother or baby. Pregnancy related complications couldn’t be reliably predicted if the mother cannot know the risk sign of child birth related [5]. Thus informing women about obstetric danger sign is among the strategies to reduce maternal mortality due to pregnancy complication [6].
Obstetric danger sign (ODS) indicates that maternal health going to wrong in related to child birth; that lead to maternal mortality and morbidity. These danger signs are mainly classified as a major danger signs in the three respective child birthing period (prenatal, childbirth, postnatal). The major danger sign includes vaginal bleeding, swollen hands/face, and blurred vision in the prenatal period, severe vaginal bleeding, prolonged labor (>12 h), convulsions and retained placenta occurred during labor and severe vaginal bleeding, foul-smelling vaginal discharge, and fever are occurring in the postnatal period are expected. Studies in Ethiopia and Tanzania shows that knowledge of women about danger signs during pregnancy, labor and postpartum are low (21.9 and 17.1-25.2%) respectively [7-9]. According to study finding Abeshige only 37.2 % of the participant were knowledgeable on birth preparedness and complication readiness, this study shows that more than 60% of the participant were going to complication due to lake of knowledge on obstetric danger sign [10]. Inadequate knowledge about danger signs of pregnancy is one of the major contributing factors for maternal deaths [11]. Therefor the purpose of this study is to identify the level of knowledge of antenatal mothers and factors about of obstetric danger signs. Increasing maternal knowledge on obstetric danger sign is an important means to reduce maternal mortality and morbidity which enable the mother to seek care before the problem arise.
Studies and reports in different parts of the world reviewed various factors associated with knowledge of obstetric danger signs. Accordingly, for this study the main factors identified are socio demographic factors like age, educational status, occupation and income. This conceptual framework was adapted by the author from the literature. Different literatures suggest that reproductive history could affect negatively and positively the KODS.
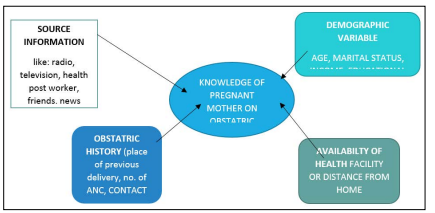
Figure 1: Conceptual framework on knowledge of obstetric danger sign and associated factors among pregnant mother
Institutional based cross-sectional study was conducted
This study was conducted in tenta woreda, governmental health institution from April 20 to May 05, 2019 and the woreda is located Debub wollo zone amhara region of Ethiopia.. Its capital city is Adjibar which is located 524 km north of Addis Ababa, 601 km from Bahirdar, and 128 kilometers from Dessie. Tenta is bordered by legambo in south, by sayint in south west, by magdala in west, by beshilo river in north and kutaber in the east The woreda has also 30 health post, nine health centers and one primary hospital. The study includes nine health center and one primary hospital which have maternity service.
Nine health center and one governmental hospitals or all health facilities in Tenta Woreda are included in the study, sample size of the study participant determined using single population proportion with prevalence of 21.9% knowledgeable on obstetric danger signs from Yirga chefe, which will be 293 ANC following mother, the sample size was allocated proportionally to nine health center and one hospital, based the information of ANC attendant of 2018, then systematic sampling was employed to select each study participant [8].
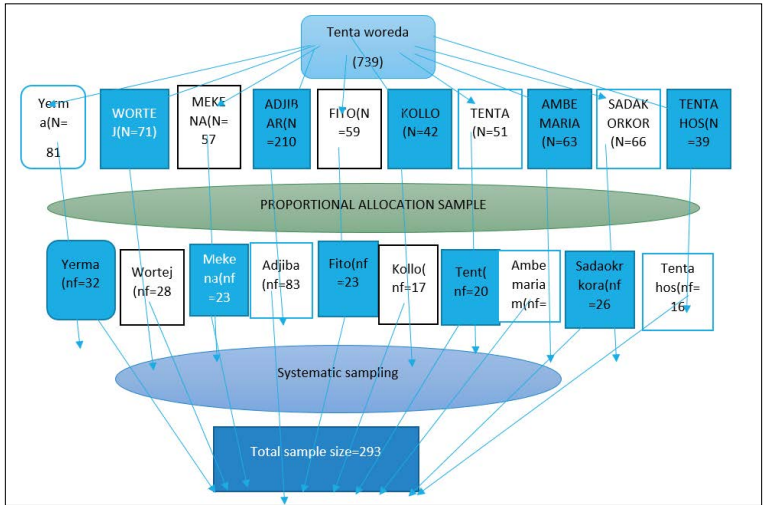
Figure 2: Schematic representation of sampling procedure for the study on knowledge of obstetric danger signs and associated factors among pregnant mothers in Tenta woreda
Structured questionnaire was adapted from the result of different previous research on KODS. Then cross cultural consistency was checked by translating English to Amharic then back to translate back to English by expert. The questionnaire has 3 parts the first part socio demographic, the second reproductive history and the third was knowledge based questionnaire about ODS. One nurse and one midwife was selected for data collection and training was given based on the plan. Data collection tool was pre-tested. Then data was collected using interviewing technique after getting individual consent, the completeness of the questioner was checked daily and correction was done Any problem, arise during the data collection process appropriate intervention was made by the principal investigator.
Training was provided for data collected based on the objective, individual consent obtained during interviewing, the Data collection tool was pre-tested in 5% of sample size at similar population in akista woreda which was not include in the study and necessary modification was done. The completeness of the collected data was check by the researcher, and necessary correction was made.
Data was entered by epi data (version 4.2.0.0) and analyzed after checking the completeness using SPSS software (version 25.0). It was coded, and cleaned before analysis. confidence interval of 95% and p- value 0.05 was used. Descriptive statistics was calculating to describe knowledge on obstetric danger signs .if the respondent mention at least three key obstetric danger signs for each of the three periods (pregnancy, delivery and postpartum) their level of knowledge well be Good, if they responded less than three leveled as poor knowledge.
Binary logistic regression done to analyze the relationship between the dependent and independent variables. Multiple logistic regression was used to analyze statistical significance because confounding variables can affect the binary logistic regression. Tables and graphs was used to present the results.
Out of the total 293 mothers who were planned for the study, 287 (98%)were responds successfully interview. The mean age of the respondents was 25.9 years (range 23 years). Most of the study participants were muslims,173 (60.3%). Majority of the respondents 255(88.9%) were married and 181 (63.1%) of them were housewife. Regarding their education 154(53.7%) of the participants had primary educational level. Partner educational status 128 (44.6 %) of respondents’ husbands did receive primary education, and 152 (53 %) were involved in farmer. About information source obstetric danger signs, 153(53.3%) got information from colloquies. (see Table 1. below)
Regarding to the obstetric characteristic 111(38.7%) respondents had history of 2-4 pregnancies and 19(6.6%) mothers were pregnant for more than four times. The other was first pregnancy. Majority, 262(81.3%) of the respondents had no history of abortion. About 50.5% of mother had health facility contact in their child bearing periods 31.1% of respondent have three and above ANC visit. (Table-2)
| Characteristics | Frequency | Percent |
|---|---|---|
| Age of respondents in year( n=287) | ||
| <20 | 45 | 15.7 |
| 21-25 | 99 | 34.5 |
| 26-30 | 84 | 29.1 |
| 31-30 | 24 | 8.2 |
| >35 | 35 | 12.5 |
| Religion( 287) | ||
| Muslim | 173 | 60.4 |
| Orthodox | 102 | 35.5 |
| Protestant | 11 | 3.8 |
| Catholic | 1 | 0.3 |
| Marital status(n=287) | ||
| Unmarried | 17 | 5.9 |
| Married | 255 | 88.9 |
| Divorce | 13 | 4.5 |
| Widowed | 2 | 0.7 |
| Occupation(n=287) | ||
| House wife | 181 | 63 |
| Civil servant | 43 | 15 |
| Farmer | 28 | 9.8 |
| Merchant | 16 | 5.6 |
| Daily labour | 19 | 6.6 |
| Educational level(n=287) | ||
| Illiterate | 52 | 18.1 |
| Primary | 154 | 53.7 |
| Secondary | 37 | 12.9 |
| Collage and above | 44 | 15.3 |
| Residency (n=287) | ||
| Urban | 89 | 31 |
| Rural | 198 | 69 |
| Paternal education(n=270) | ||
| Illiterate | 40 | 14.8 |
| Primary | 128 | 47.4 |
| Secondary | 63 | 23.3 |
| Collage and above | 39 | 14.5 |
| Paternal occupation excluded the unmarried(n=270) | ||
| Civil servant | 31 | 11.5 |
| Farmer | 152 | 56.3 |
| Merchant | 71 | 26.3 |
| Daily labour | 16 | 5.9 |
| Monthly income in birr in birr( n=287) | ||
| 0-600 | 93 | 32.4 |
| 601-1650 | 95 | 33.1 |
| 1651-3200 | 48 | 16.7 |
| >3201 | 51 | 17.8 |
| Distance from home to the nearest HF in minute (n=287) | ||
| 10-65 | 176 | 61.3 |
| 66-121 | 92 | 32.1 |
| 122-180 | 19 | 6.6 |
| In case of getting information about ODS for alternative (n=287) | ||
| From health personnel | 104 | 36.3 |
| From media | 99 | 34.5 |
| From family | 97 | 33.8 |
| Colloquies | 153 | 53.3 |
| From school | 24 | 8.4 |
From the total number of.
| Characteristics>Previous obstetric characteristics |
Characteristics>Frequency | Characteristics>Percent |
|---|---|---|
| Number of pregnancy (n=287) | ||
| 1 | 157 | 54.7 |
| 2-4 | 111 | 38.7 |
| >=5 | 19 | 6.6 |
| Number of follow up in this pregnancy (n=287) | ||
| 1 | 131 | 45.6 |
| 2 | 61 | 21.3 |
| 3 | 56 | 19.5 |
| >=4 | 39 | 13.6 |
| ANC in previous pregnancy for those history of previous pregnancy(n=130) | ||
| yes | 84 | 64.6 |
| No | 46 | 35.4 |
| Previous place of delivery for those history of previous delivery(n=122) | ||
| health facility | 45 | 36.9 |
| Home | 38 | 31.1 |
| Health facility and home | 39 | 32 |
| history of abortion(n=287) | ||
| Yes | 25 | 8.7 |
| No | 262 | 91.3 |
| previous health facility contact (n=287) | ||
| Yes | 145 | 50.5 |
| No | 142 | 49.5 |
This study identifies that 44.6% (128) of the participant were Knowledgeable about obstetric danger signs during prenatal period and 55.4%(159) mothers were found to be not knowledgeable about danger sign during pregnancy. Most of the respondents (71.4%),32.4 % knew that vaginal bleeding and reduce fetal movement are danger sign during pregnancy sequentially. And 11.2%(33) were no listed any perinatal danger signs. (Table three below)
| Respondent’s knowledge on obstetric danger sign during pregnancy(n=287) |
||
|---|---|---|
| Danger sign | Number of respondents who list pregnancy danger sign |
Percent |
| Vaginal bleeding | 205 | 71.4 |
| Lag and face edema | 66 | 23 |
| Blurring of vision | 63 | 22.4 |
| Severe headache | 46 | 16 |
| Loss of consciousness |
35 | 12.2 |
| Difficult of breathing |
39 | 13.6 |
| Severe weakness | 51 | 17.8 |
| Severe abdominal pain |
52 | 18.1 |
| Reduce fetalmovement |
93 | 32.4 |
| Water break before labour |
44 | 15.3 |
| Malodorous vaginal discharge |
36 | 12.5 |
| Persistent back pain |
66 | 23 |
| Persistent vomiting |
94 | 32.8 |
Out of 287 respondents 140 (48.8%) were have adequate knowledge, but 147(51.2%) of women were found to be not knowledgeable about danger sign during labor. Majority of the respondents (76.0%) 39.4%, 31% knew that Severe vaginal bleeding, retained placenta and cessation of labor are identified danger sign related to child birth period respectively. 22(7.7%) were no listed any danger sign that probably occurs during delivery (see the table below)
| Respondent’s knowledge on obstetric danger sign during child birth (n=287) | ||
|---|---|---|
| Danger sign | No. ofrespondentwho list labour danger signs |
Percent |
| Severe vaginal bleeding |
218 | 76 |
| Coming of cord before head |
72 | 25.1 |
| Labour lasting more than 12 hrs. |
32 | 11.1 |
| Convulsion | 48 | 16.7 |
| Water break more than 8hrs |
27 | 9.4 |
| Malpresentation | 68 | 23.7 |
| Retained placenta | 113 | 39.4 |
| Persistent severe abdominal pain |
63 | 22 |
| High fever | 45 | 15.7 |
| Cessation of labour |
89 | 31 |
From a total of 287 respondents, 132(46.0%) were knowledgeable and 155 (54.0%) study participants were found to be not knowledgeable about danger sign during postpartum period. Most of the respondents (71.8%) knew that severe vaginal bleeding is a danger sign during postpartum period. Severe abdominal pain, face and lag edema and sever weakness are repeatedly listed danger sign during postnatal and 29(10.1%) respondents were no listed any danger sign as shown the table below.
| Respondent’s knowledge on obstetric danger sign during postnatal (n=287) | ||
|---|---|---|
| Danger signs | No. ofrespondent who list postnataldanger sign | Percent |
| Severe vaginal bleeding | 206 | 71.8 |
| Abdominal pain | 96 | 33.4 |
| Fever | 54 | 18.8 |
| Offensive vaginal discharge | 37 | 12.9 |
| Convulsion | 52 | 18.1 |
| Severe weakness | 81 | 28.2 |
| Blurring of vision | 70 | 24.4 |
| Lag and face edematous | 96 | 33.4 |
| Uterine prolapse | 59 | 20.6 |
| Cessation of labour | 89 | 31 |
The knowledge of obstetric danger signs in combination of the three priods (prenatal, labor and child birth and postnatal period) as shown the figure below
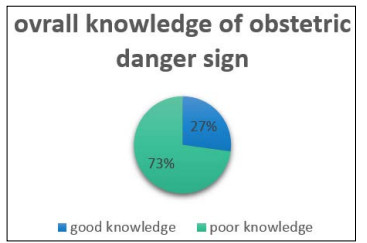
Figure 3: The Knowledge of Pregnant Mother on Obstetric Danger Sign in Combination of Prenatal,Child Birth and Postnatal in Tenta Wored, Ethiopia, 2019
Over all knowledge of participants that who list a minimum of three obstetric danger signs from each child bearing period (perinatal, child birth and postnatal) from Crude odd ratio indicates that the age of pregnant mothers had an impact for maternal knowledge on obstetric danger signs, being maternal age 31-35 has seven times knowledgeable than age less than 20 (COR=7.32,95% CI=1.98,27.1) Maternal educational status was significantly associated with knowledge about obstetric danger signs. Respondents who had a secondary education level had almost five times knowledgeable, (AOR=4.7 and 95% CI=1.00,32.01) than illiterate. The study showed that mothers, who worked as civil servant, were about 9.8 times more knowledgeable about danger signs of pregnancy than housewives, (AOR=9.8 and CI=1.53,62.997).
Frequency of Antenatal care (ANC) visit was significantly associated with knowledge respondents about obstetric danger signs. Mothers having four ANC follow-ups were thirteen times knowledgeable about obstetric danger signs than mothers having only one visit. Residence were an effect on the knowledge of mothers about obstetric danger signs, participants who were leave in urban area were three times knowledgeable than participants who leave in rural area AOR=3.1, and 95%CI=1.059, 9.34).
Health facility contact would increase the knowledge of health related problem, respondents who had previous health facility contact related to their health had eleven times knowledgeable than those who had no contact rather than the current pregnancy checkup (AOR=11.3, 95% CI=3.756,34.11) as shown in the table below
This study aimed to assess maternal level of knowledge on obstetric danger sign and associated factors Among Pregnant Women Attending Antenatal Care At Health Facilities, In Tenta Woreda, South Wollo, Ethiopia 2019.
In this study of three periods (prenatal period, child birth and postnatal period) repondan were reputedly mention the key danger sign were 78(27.2%). This finding is almost in line with the study finding in Yirgachefe (21.9%) [8]. The similarity is may be due to almost similar, education level, pregnancy history, health facility contact. This finding was also higher than the study finding in errer, Somalia (15.5%), Uganda (18.7) and lower than the study finding in Debaytilatgin (56.8), mamprusi, Ghana (51.1) [12,13,14,15]. The variation is may be the population difference of the study unit in which the study were conducted reproductive age group, the health related strategy difference specially the studies those out of Ethiopia.
Below half of the respondents were, 128 (44.6%) knowledgeable about danger sign during pregnancy. This finding is consistent with the study conducted in Raya kobo, (46.7%), India (49.2) in which respondents mentioned at least three danger signs of pregnancy [16,17]. But higher than the study finding in Goba district, Ethiopia (31.9) [18]. the difference is may be due to the study participant’s education level, the residence of participants, the previous pregnancy difference of participants, the health professional awareness difference.
From the women under the study, 140 (48.8%) were knowledgeable about danger signs during child birth. This finding was higher than the study finding in Raya, (27.8%), Goba district (27%) [17,18]. The difference is may be due to the participant’s education level, the study population, and the reproductive history difference and the health education of professional’s.
Additionally, 132 (46%) were knowledgeable about danger signs during postpartum period which is consistent with similar study in Yirgachefe (44.7%) in which women know at least three danger signs during postpartum period [8]. The finding were not consistent with the study in Uganda (71.6%) [13]. This difference might be due to variation in sociodemographic aspect, particularly education level, the residency of respondents.
In the current study, Vaginal bleeding was the frequently listed obstetric danger sign during prenatal 205 (71.4%), labor 218 (76%), and postpartum period, 206 (71.8%). So it is less likely listed from the finding in Raya kobo,(83.5%) in prenatal, (91.2%) in child birth and (89.2%) in postpartum [17]. This could be an indication of awareness difference for women that bleeding is the main and fastest cause of maternal mortality. Blurring of vision 64(22.3), leg and face edema 66 (23%) and convulsion has listed by16.7 % were the obstetric danger signs mentioned by the study participants. These findings were consistent with the study conducted in chamwino, Tanzania, which had 20.6%, 20.1% and 15.9% in blurred of vision, swallow of leg and face and convulsion respectively( [9]. This similarity was might be due similarity in the study design
Regarding to the factors in which independently associated with knowledge of obstetric danger signs, participants who had secondary education level were 4.7 times knowledgeable about obstetric danger sign than illiterate (AOR=4.7, 95% CI=1.00,22.01). this finding was in line with the study conducted in in Tanzania, AOR=1.96, and Raya kobo, AOR=3.63 [9,17]. This is the fact that education was one instrument to increase the understanding ability of maternal fitness to knowledge. Also, knowledge of obstetric danger signs were ten times higher among civil servant women compared to house wife (AOR = 9.8, 95% CI=1.53,62.997).This finding were consistent with the study finding in Goba district [18].
| Independentvariable | GoodknowledgeN(%) | Poor knowledge N(%) | COR (95% CI)overall knowledge on ODS | P-value | AOR (95% CI)overall knowledge on ODS | p-value |
|---|---|---|---|---|---|---|
| Age | ||||||
| >20 | 4(8.9) | 41(91.1) | 1 | 1 | ||
| 21-25 | 24(24.2) | 75(75.8) | 3.28(1.06,10.1) | 0.038 | 3(.941,9.85) | 0.063 |
| 26-30 | 32(38.1) | 52(61.9) | 6.3(2.06,19.277) | 0.001 | 1.448(0.391,5.34) | 0.579 |
| 31-35 | 10(41.7) | 14(58.3) | 7.32(1.98,27.1) | 0.003 | 0.625(0.10,3.85) | 0.602 |
| >36 | 8(22.9) | 27(70.1) | 3.03(0.83,11.02 | 0.093 | 0.439(0.077,2.51) | 0.356 |
| Religion | ||||||
| Muslim | 37(21.4) | 136(78.6) | 1 | 1 | ||
| Orthodox | 36(35.3) | 66(64.7) | 2(0.20,3.42) | 0.12 | 1.4(0.638,3.13) | 0.394 |
| Protestant | 4(36.4) | 7(63.6) | 2.1(0.58,7.56) | 0.256 | 0.47(0.043,5.16 | 0.538 |
| Catholic | 1 | 0 | Xx | Xx | ||
| Occupation | ||||||
| House wife | 25(13.8) | 156(86.2) | 1 | 1 | ||
| Civil servant | 36(83.7) | 7(16.3) | 32(12.8,79.97) | 0.000 | 9.8(1.53,62.997) | 0.016 |
| Farmer | 5(18.9) | 23(81.1) | 0.57(0.47,3.89) | 1.357 | 0.879(0.246,3.14) | 0.843 |
| Merchant | 12(75) | 4(25) | 18(5.59,62.639) | 0.000 | 2.46(0.265,22.8) | 0.429 |
| Daily labor | 0 | 19 | 0.124(0.016,0.95) | 0.16 | 0.115(0.009,1.4) | 0.09 |
| Educational status | ||||||
| Illiterate | 5(9.6) | 47(90.4) | 1 | 1 | ||
| Primary | 16(10.4) | 138(89.6) | 1.09(0.38,3.137) | 0.87 | 6.38(1.78,22.9) | 0.005 |
| Secondary | 23(62.2) | 14(37.8) | 15(4.95,48.110) | 0.000 | 4.7(1.00,22.01) | 0.049 |
| Collage and | 34(77.3) | 10(22.7) | 31.9(10.02,102.5) | 0.000 | 3.28(0.39,27.774) | 0.277 |
| Collage andabove |
34(77.3) | 10(22.7) | 31.9(10.02,102.5) | 0.000 | 3.28(0.39,27.774) | 0.277 |
| Marital status | ||||||
| Unmarried | 2(11.8) | 15(88.2) | 1 | 1 | ||
| Married | 73(28.6) | 182(71.4) | 3(0.67,13.48 | 0.15 | 0.18(0.026,1.25) | 0.083 |
| Divorce | 2(15.4) | 11(84.6) | 1.36(0.166,11.233 | 0.773 | 0.007(0.00 , 0.192) | 0.003 |
| Widowed | 1 | 1 | Xx | xx | xx | Xx |
| Monthly income in birr | ||||||
| 0-600 | 7(7.5) | 86(92.5) | 1 | 1 | ||
| 601-1650 | 18(18.9) | 77(81.1) | 2.87(1.138,7.247) | 0.025 | 1.5(0.610,3.75) | 0.37 |
| 1651-3200 | 18(37.5) | 30(62.5) | 7.37(2.8,19.38) | 0.000 | 4(1.34,12.17) | 0.013 |
| >=3201 | 35(68.6) | 16(31.4) | 26.9(10.18,70.98) | 0.000 | 6.3(1.3,30.55) | 0.021 |
| Residence | ||||||
| Rural | 20(10.1) | 178(89.9) | 1 | 1 | ||
| Urban | 58(65.2) | 31(34.8) | 16.6(8.8,31.44) | 0.001 | 3.1(1.059,9.34) | 0.039 |
| No. of follow up | ||||||
| First | 14(10.7) | 117(89.3) | 1 | 1 | ||
| Second | 4(6.6) | 57(93.4) | 0.56(0.185,1.89) | 0.365 | 3.8(1.535,9.55) | 0.004 |
| Third | 36(64.3) | 20(35.7) | 15(6.90,32.76) | 0.000 | 8.7(2.09,36.319) | 0.003 |
| >=fourth | 24(40) | 36(60) | 13.4(5.71,31.3) | 0.002 | 12.8(1.28,128.39) | 0.03 |
| Gravidity | ||||||
| I | 34(21.7) | 123(78.3) | 1 | 1 | ||
| II-IV | 38(34.2) | 73(65.8) | 1.88(1.09,3.25) | 0.023 | 0.847(0.32,2.22) | 0.736 |
| >=V | 6(31.6) | 13(68.4) | 1.67(0.59,4.72) | .334 | 5.2(0.89,30.3) | 0.067 |
| Gate information from health personnel | ||||||
| Yes | 72(49.7) | 73(50.3) | 22(9.27,53.9) | 0.000 | 11.3(3.756,34.11) | 0 |
| No | 6(4.2) | 136(95.8) | 1 | 1 | ||
| From Media | ||||||
| Yes | 71(68.3) | 33(31.7) | 54(22.87,127.9) | 0.000 | 1.7(1.705,19.22) | 0.032 |
| No | 7(4.8) | 176(95.2) | 1 | |||
| From Media | ||||||
| Yes | 66(66.7) | 33(33.3) | 29(14.29,60.19) | 0.000 | 2.12(7.80,12.3200 | 0.004 |
| No | 12(6.4) | 176(93.6) | ||||
Women who live in urban area were three times more likely to mention at least three obstetric danger signs as compared with rural counterparts (AOR=3.1, and 95%CI=1.059,9.34). This variable was also found to have a significant association with other study conducted in Goba district, yirgachefe and erere, Somalia [8,18,15]. This could be due to the fact that urban residents have better access to health information and maternal health services as compared with rural counterparts. Multivariate regression indicates that increase the number of Antenatal care follow up also increase the maternal knowledge on obstetric danger signs, participants who had four or more visited were 13 times knowledgeable on obstetric danger sign than one visitor, (AOR=12.8, 95%CI=1.28,128.39) this finding was in line with the study finding in Debaytilatgin, AOR=3.46 [12]. In the binary logistic regression, analysis revealed that, adequate ANC follow up, women education, occupation, parity, income, and number of ANC, age, residence were found to be an independently significant association with knowledge of obstetric danger signs. This finding was congruent with the study finding in Debaytilatgin [12]. This similarity may be due to all most similar sociodemographic aspect, health issue related policy [19-25].
The limitations of this study could be the small sample size which may make estimates unstable and associations between dependent and independent variables undetectable. The method cross sectional was another limitation, in which able to detect cause and effect
In current study a significant proportion of mothers were not knowledgeable about the danger signs of pregnancy, labor and childbirth and postnatal. This indicates that many women not likely to seek health care during antenatal labor and postnatal period. Sever Vaginal bleeding was the most common spontaneously mentioned danger signs among the three periods. According to the result of this study, age, level of education, occupation, residence, health facility contact, antenatal care follows up were the predictors association factor for knowledge of mothers about obstetric danger signs during pregnancy, labor and post-partum period. Therefore, intervention programs aiming to improve women’s knowledge about obstetric danger signs in the area of health facility, Federal ministry of health and research area.
By my signature below, I declare and affirm that this thesis is my own work. I have followed all ethical principles of scholarship in the preparation, data collection, data analysis and completion of this thesis.
Ethical clearance was received from AAU college of Health science, school of nursing and Midwifery research team prior to data collection. A formal letter was written by the department of nursing to the concerned office. Permission were asked from the responsible body of the unit. Each study participant was adequately informed about the purpose, methods, and anticipated benefits of the study by the data collectors. Respondents who were volunteer and was available at the time of data collection were interviewed without writing their names to ensure confidentiality. Used reference materials for the study was coated and cited with their proper Authors, funding organization, the study subject, the institution, advisors and people supporting in searching literature (digital Liberian,) data collector, supervisors and all peoples contribute genuine suggestion and advise was duly acknowledged.
not necessary
All the information or data incorporated in the manuscript can be accessed primary author and other co-author with the email address of mohalegas86@gmail.com
No competing interest since the author declare
This study funded by Addis Ababa university student grant of post graduate office, which is small to cover the wholly process the study activity
Legas Mohamed develop the proposal, search literatures, select and train the data collector, analysis and wrote the finding and discussion
Teshom R, and Abebe WS advising on starting from the development of proposal and to defending time about methodological,reviewing ,writing result and analysis issue
We are indebted to addis ababa university college of health scince school of nursing and midwifery in giving both financial and technical support, we also our great thank to Tenta woreda health bureau helping for the entire process of the research is successful. Our special thank goth to the participant and technical assistant in the data collection process.