Author(s): Huang Chun-Yi, Yu Jian-Hong*, Lin Chih-Chieh, Lo Yu-Cheng and CHEN Yuan-Hou
Patients with a Class II malocclusion, proclination, severe crowding of the maxillary and mandibular anterior teeth, and high mandibular plane angles are a treatment-planning challenge. This case report describes an orthodontic treatment and maxillary premolar extraction without orthognathic surgery for a 18-year old man. Maximum anchorage is needed for upper anterior retraction by using a Temporary Anchorage Device (TAD’s). The use of IME and ISW unilateral MEAW was important to relieve upper and lower anterior crowding. After treatment, the patient had a better profile, adequate overjet and overbite. This case report demonstrates that a minimally invasive treatment can successfully correct a severe skeletal Class II malocclusion with large overjet.
An Angle Class II malocclusion with a skeletal Class II profile is a major reason that a patient sought for orthodontic treatment. Severe Class II with large overjet in an adult is a difficult problem for orthodontists to correct [1]. Treatment protocols can widely vary according to malocclusion severity, clinical experience and patient compliance [2]. The most effective treatment option for patient with dental and skeletal malocclusion requires a surgical approach [3]. However, when a patient strongly refused surgery, non-surgical orthodontic approach becomes an alternative. Such a treatment should effectively maintain extraction space for anterior retraction and achieve a better profile without surgical intervention. To reinforce anchorage, many auxiliaries can be used, including headgear, transpalatal arch(TPA) and intermaxillary elastics [4]. These appliances help to achieve acceptable results with good patient cooperation. It’s difficult to establish maximum anchorage for anterior retraction with traditional orthodontic mechanics. Temporary Anchorage Device (TAD’s) was recently developed to correct such kinds of severe malocclusions. Even though in lack of patient cooperation, TAD’s can provide stable anchorages for various tooth movements. Anterior retraction with TAD’s is a new strategy for treating skeletal Class II patients [5,6].
University Hospital in Taiwan for an orthodontic consultation. No specific medical problems or temporomandibular joint symptoms were observed. At the time of his initial visit, he came with a chief complaint of poor dental alignment and for esthetic consultation. He had a severe skeletal Class II relationship and large overjet, with a short chin deviated to the left. A Class II molar relationship on the right and left, anterior crowding, lip postured to seal and open bite were observed (Fig 1). Model analysis showed bilateral Class II molar and canine relationships with an overjet of 9.0 mm, arch length discrepancy of -9.0 mm on the upper arch and -13.0 mm on the lower arch, and a midline shift of the mandibular arch (Fig 2).
A panoramic film radiograph showed bilateral horizontal impacted third molars in the mandible and showed bilateral maxillary third molars. Initial lateral and posteroanterior cephalometric radiographs were taken in centric occlusion with closed lips. The cephalometric analysis demonstrated a severe Class II relationship (ANB angle, 9.0°), high mandibular plane angle (FMA angle, 48.9°) and large lower facial height due to the maxillary excess.


Figure 1: Pretreatment facial and intraoral photographs
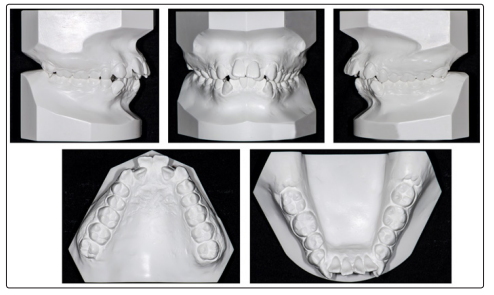
Figure 2: Pretreatment dental casts

Figure 3: Pretreatment lateral and frontal cephalograms and panoramic radiograph
Table 1: Comparison of cephalometric measurements| Measurements | Pretreatment | Pretreatment |
|---|---|---|
| SNA | 78.5 | 78.0 |
| SNB | 69.5 | 69.3 |
| ANB | 9.0 | 8.7 |
| FMA | 48.9 | 47.9 |
| U1 to FH plane | 113.1 | 100.1 |
| IMPA | 93.8 | 101.4 |
| Interincisal angle | 104.1 | 110.6 |
ISW (Improved Super-elastic Ti-Ni alloy wire, developed by Tokyo Medical and Dental University) was used for management of the 18-year-old patient presenting with a large overjet, maxillary protrusion and anterior crowding of the teeth in the upper and lower jaws. The treatment objective was to achieve a better interdigitation, adequate overbite and overjet.
Our treatment objectives were to improve the patient’s facial profile, to accomplish desirable anterior occlusion for establishing functional occlusion, to correct the midline deviation, and to follow up the retention so as to assess the need for further treatment [1-4].
There were three treatment alternatives presenting to the patient.
After we discussed the treatment alternatives with the patient, he was reluctant to undergo surgery and thus selected the second option for improvement of his facial profile and occlusion.
Before orthodontic treatment, maxillary premolar and four third molars were extracted. Initial leveling progressed over maxillary arch with 0.016-inch x 0.022-inch ISW (Fig 4). Crimpable hooks were placed at the distal side of canine. Canine distal drive with 100gf of improved super-elastic nickel-titanium alloy closed coil springs from crimpable hooks to first molar bilaterally was performed at the same time. Three months after the start of treatment, brackets were bonded over the lower arch and leveling with 0.016 x 0.022 ISW
Seven months later, maxillary anterior retraction started. Gable bend was added at the distal side of maxillary lateral incisor to avoid anterior teeth lingual tipping while torquing the roots in. Serial ligature tying (SLT) was performed over maxillary four incisors (Fig 5). Long crimpable hooks were attached at the anterior portion of gable bend, and elastic chain was applied between long crimpable hooks and maxillary first molar.
After anterior retraction, patient still complained of facial profile. And therefore, TAD’s were installed at the maxillary arch with a 1.5x8 mm dual threaded mini-implant so as to provide stable anchorage. Distalization of maxillary arch was started with elastic chain and TAD’s (Fig 6). The same progression was done at the lower arch after distalizatoin of maxillary arch was done.
In the 29th month of treatment, the retraction of anterior teeth met the pretreatment goal. Fnishing and detailing stage was started with intermaxillary elastics, which were applied from right maxillary canine to right mandibular canine and from left maxillary canine to left mandibular first premolar (Fig 7). ISW unilateral MEAW was performed at the maxillary right arch for midline correction (Fig 8). After 48months of orthodontic treatment, active treatment was finished, and all fixed orthodontic appliances were removed. Circumferential retainers were placed over the upper arch and Hawley retainer over the lower arch. The instructions to the patient included full-time retainer use for 3 months and then night-wear only for 2 years at least.

Figure 4: Intra-oral photographs during initial alignment

Figure 5: Intra-oral photographs when anterior retraction was started

Figure 6: Intra-oral photographs after anterior retraction

Figure 7: Intra-oral photographs during fnishing and detailing stage

Figure 8: Intra-oral photographs during midline correction
The final records (Fig9-11) showed that the patient’s dental problems were apparently improved through orthodontic treatment with TAD’s. Anterior crowding was relieved, and the dental midline was coincident. The space from extraction was totally used for anterior retraction. The post-treatment photographs showed an attractive smile. Although the lower anterior facial height and chin position had changed little, the protrusion of both lips and the mentalis strain upon closure were eliminated. The molar relationship remained in Class II but adequate overbite and overjet were achieved.
The post-treatment cephalometric and panoramic radiographs showed the treatment goals were basically accomplished. The maxillary anterior teeth were retracted about 9.0 mm at the incisal edge. The amount of counterclockwise rotation of the mandible was less than predicted before treatment (Table 1). The panoramic radiographs show well-aligned root parallelism of the teeth, but some root shortenings were observed in the maxillary anterior teeth
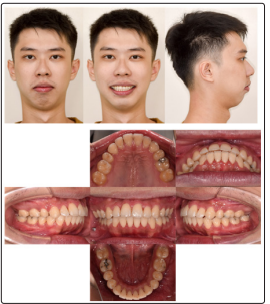
Figure 9: Post-treatment facial and intraoral photographs
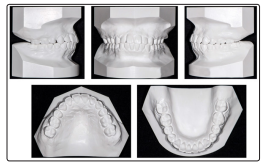
Figure 10: Post-treatment dental casts

Figure 11: Post-treatment lateral and frontal cephalograms and panoramic radiograph
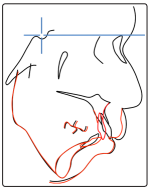
Figure 12: Superimposition of the lateral cephalograms at pretreatment (black) and posttreatment (red)
The crucial part of the maxillary and mandibular anterior crowding with open bite caused further esthetic concern for this patient. After active treatment, these orthodontic problems were satisfactorily relieved through retraction of maxillary anterior teeth and elimination of the bimaxillary protrusion. The upper lip became more relaxed and was placed backward, which allowed the patient to close his lips more easily.
Early treatment for severe Class II high-angle patients offered no skeletal or dental advantage over the late treatment [7]. For our patient, the pre-treatment analysis indicated that the factors associated with his abnormalities seemed to be excessive maxillary growth and protrusion. Orthognathic surgery is generally needed to treat these skeletal problems. However, when a patient strongly refused to receive surgery, retraction of maxillary anterior teeth and maximum anchorage were commonly planned for this treatment.
Therefore, the first choice of correcting the anterior crowding was performed mainly through flaring out the anterior teeth. However, these patients had skeletal Class II with open bite, maxillary teeth flaring out may worsen protrusion of the lips and could produce a convex facial profile. Therefore, improvement of the profile and arch coordination can be obtained by tooth extraction to relieve the skeletal discrepancy. The decision of extraction sites is a key judgment in designing orthodontic treatment procedures. The maxillary first premolar and mandibular second premolar extraction protocol is an acceptable method of gaining the required space for patients who might benefit from it. The ultimate decision of whether to extract mandibular second premolar is made by the clinician. After leveling, we decided not to extract mandibular second premolars to prevent the mandibular arch from becoming smaller, especially for those cases with severe Class II malocclusion, particularly when existing with anterior crowding. However, the orthodontic treatment frequently became more complicated and time-consuming than expected at the start.
ISW has been developed with unique characteristics that offer significant potential for orthodontic appliances. ISW offers three main significant properties characterized by super-elasticity, shape memory, and shock and vibration absorbing properties according to the results by Dr. Iramaneerat showed that high damping capacity of ISW had an ability to buffer the transmission of occlusal forces to the PDL [8,9]. When lighter forces are transmitted to the roots of the teeth, there is less patient discomfort and root resorption [10]. With ISW unilateral MEAW, we can effectively tip the mandibular molars distally and can correct the midline. The MEAW technique and Class II elastics provided an appropriate treatment strategy especially for patients with high angle and open bite tendency
In this case, facial profile and dental alignment were greatly improved. The use of TAD’s, IME and ISW unilateral MEAW was very important to solve the large overjet and correct midline. A more harmonious smile arc of the patient was achieved at the end of the treatment. As a result, the patient was satisfied with the treatment outcome and pleased with his face appearance change.
This patient had Class II malocclusion with large overbite, overjet and severe anterior crowding. He was treated successfully with extraction of maxillary premolars and the mechanism of unilateral MEAW and Temporary Anchorage Devices. By using Temporary Anchorage Devices, we successfully secured the extraction space for crowding relief and anterior retraction. As a result, a desirable outcome was achieved and the patient was pleased with the treatment result. With this successful experience, orthognathic surgery may not be the only one choice in patients with severe Class II. Minimally invasive treatment can be planned for a patient with slight facial asymmetry and severe lower anterior crowding