Author(s): <p>Areeg Abd-Alaziz Alnoor Mohammed, Amira Altoom Fuzi Othman and Babbiker Mohammed Taher Gorish<sup>*</sup></p>
Patients with cancer are particularly under risk of many microbial infections and even septicaemia due to the weakened immune system induced by Chemotherapy. This study was done to identify and isolate aerobic bacterial septicaemic pathogens among cancer patients. This study was performed in Radiation and Isotopes national Centre of Khartoum Hospital (previously Alzarra) during the period from September to November 2019. One Hundred Fifty blood samples were collected from cancer patients suspected to have septicemia. All samples where inculated in blood culture media and incubated aerobically. Upon detection of growth signs the bacterial isolates were subcultured and identified according to the Standard known procedure. Antimicrobial sensitivity test was done following CLSI guidelines, The study showed that Twenty two (14%) of the investigated samples were showed growth signs, while One hundred Twenty eight (86%) were showed no growth. After subculture on Blood agar, MacConky agar and Chocolate agar, all isolated pathogens were subjected to essential acteriological biochemical tests and identified as E.coli (57.1%) , Klebsiella pneumonia (19%) ,Staphylococcus aureus( 9.5%), Pseudomonas aeruginosa (4.8%) . Citrobacter Spp (4.8%) and Streptococcus pyogens (4.8%). Septicaemia in patients with cancer was mainly caused by E.coli in patients using chemotherapy. Further study with inclusion of more sample size and focusing on multidrug resistant isolates is essential to verify the current study results.
Cancer is the name given to a collection of related diseases. In all types of cancer, some of the body's cells begin to divide without stopping and spread into surrounding tissues, it can start almost anywhere in the human body, which is made up of trillions of cells. Normally, human cells grow and divide to form new cells as the body needs them. When cells grow old or become damaged, they die, and new cells take their place [1]. The Globcan 2018 estimates of cancer incidence and mortality produced by the International Agency for Research on Cancer, with a focus on geographic variability across 20 world regions. There will be an estimated 18.1 million new cancer cases (17.0 million excluding non-melanoma skin cancer) and 9.6 million cancer deaths (9.5 million excluding non-melanoma skin cancer) in 2018 [2]. For cancer patients an infection can turn serious or even deadly, very fast. Sepsis is a complication caused by body's overwhelming and life-threatening response to infection, which can lead to tissue damage, organ failure and death.
Sudan is experiencing a growing cancer problem, but little is presently known on tumor patterns, cancer epidemiology and ethnic or environmental cancer risk factors. According to the data from local and international publications as well as primary information from the only two cancer hospitals of the country, both located in Central Sudan (Khartoum and Wad Medani).The cancer prevalence rate per year was 5,000-7,000 among adults and 300-400 among children, with increasing tendency for adults. Male: female ratios were 1:1.18 for adults and 1.46:1 for children. Comparing cancer cases with population numbers of Sudanese states, Northern Sudan, River Nile and Khartoum revealed up to 8-fold higher cancer incidence rates than Al Gedarif, Southern Dafur and Blue Nile [3-5].
People with cancer are particularly susceptible to developing bacteremia and sepsis [4]. An American study published in 2004 found that patients with cancer were much more likely to be hospitalized with severe sepsis (the stage just before septic shock) than the general population. The study also found that severe sepsis caused 8.5 percent of cancer-related deaths and cost over three billion dollars a year to fight [6,7].
The laboratory detection of bacteremia remains one of the most important functions of clinical microbiology laboratories. A positive blood culture establishes or confirms that there is an infectious etiology of the patient's illness. Using blood cultures is one of the most simple and commonly used investigations to establish the etiology of bloodstream infections. Microorganisms causing bloodstream infections are highly varied (aerobes, anaerobes, fungi, fastidious microorganisms) and, in addition to nutrient elements, may require specific growth factors and/or a special atmosphere . In cases where the patient is receiving antimicrobial therapy, specialized media with antibiotic neutralization capabilities should be used [8]. Antibiotic neutralization media have been shown to increase recovery and provide faster time to detection versus standard media [8].
The laboratory detection of bacteremia remains one of the most important functions of clinical microbiology laboratories. A positive blood culture establishes or confirms that there is an infectious etiology of the patient's illness. Using blood cultures is one of the most simple and commonly used investigations to establish the etiology of bloodstream infections. Microorganisms causing bloodstream infections are highly varied (aerobes, anaerobes, fungi, fastidious microorganisms) and, in addition to nutrient elements, may require specific growth factors and/or a special atmosphere . In cases where the patient is receiving antimicrobial therapy, specialized media with antibiotic neutralization capabilities should be used [8]. Antibiotic neutralization media have been shown to increase recovery and provide faster time to detection versus standard media [8].
This study was across-sectional study to determine the prevalence of an aerobic bacterial pathogens from blood culture of cancer Patients .The study was conducted in Radio Isotope center of Khartoum state (Al Zara Hospital) between the periods from September to November 2019.
Cancerous patients with different age and gender were included in this study.
Patients confirmed to have cancer were included in this study regardless the age, gender and presence or absence of sepsis symptoms. Any patients referred to hospital with at Atpia or not confirmed to have a cancer were excluded from this study
Simple random sampling technique was used to collect 150 blood samples from patients with different kinds of cancer in Alzera Hospital. Blood samples were collected from each individual patient according to the guidelines of aseptic blood collection [9]. The volume of blood was decided depending on the age of patient in which 5-10 ml was assigned for adult while children were 2.5 to 5 ml blood samples (following blood culture media direction) [9,10].
The blood samples were cultured immediately on blood culture media bottle (Tryptic soy broth) following the direction of volume. This was preceded by changing the syringe which was used to collect the blood by other sterile syringe. Then the blood was added to the bottle after decontamination of the rubber part by alcohol. Then the bottle which holding the blood will be gently mixed and incubated
The incubated bottle was monitored for the presence of bacterial growth signs. If there is no signs of growth the bottle was been sub cultured each twice days up to 7 and days. The appearance of that signs will followed by and the subculture by using sterile syringe and calibrated loop (500μm in diameter) on to blood agar , chocolate The incubated bottle was monitored for the presence of bacterial growth signs. If there is no signs of growth the bottle was been sub cultured each twice days up to 7 and days. The appearance of that signs will followed by and the subculture by using sterile syringe and calibrated loop (500μm in diameter) on to blood agar , chocolate
The isolated organism was subjected to the antimicrobial sensitivity test by using sterile Muller- Hinton agar plate and appropriate antimicrobial agent followed by incubation In appropriate temperature. Zone of inhibition was measured after overnight incubation. The interpretation chart was used to interpretate the result of sensitivity test as sensitive, resistant and intermediate.
Structured questionnaire was used to ask the patients about their age, gender as well as their cancer type.
Data was analyzed by computerized method (Statistical Package for Social Sciences) (SPSS version 20). Special test such as Independent T-test, Chi squire test was used to assess the effect of gender on the blood culture results and type of isolate
All culture media that was used in this study will checked for sterility by incubation for overnight without adding any specimen. ATCC strain was used to confirm the stability of the growth component of the culture media and the potency of antibiotic. The procedure of Isolation, Identification and sensitivity tests were done under aseptic condition to reduce the possible contamination. Incubator temperature and aeration were also be checked.
Before conducting the study, the proposal of the study was ethically approved by the ethical committee of Alzaeim Alazhary University. Then informed consent from each patient and permission from the general managers of hospitals were obtained.
In this study, a total of 150 blood samples were investigated, 150 blood samples were collected from cancer patients . The mean age of study participants was 42.5 years. Significant bacterial growth was detected 14 blood samples (14 %) (Figure 1). The highest percentage of the infection was found in the outpatients with (64%). And the lowest frequency was observed in the Residence patients (36) (Figure 2) with no relationship and no significant difference (P=.245). A slightly highest rate of growth in Male with (11 %) in compare to Female with (10 % ) with no significant difference (P= .814) (Figure 3). The commonest organism isolated is detected: E.coli (57.1%), Klebsiella pneumonia (19%), Staphylococcus aureus (9.5%), and Pseudomonas aeruginosa (4.8%). Citrobacter Spp (4.8%) and Streptococcus pyogens (4.8%) (Figure 4). Antimicrobial drugs resistance for the Bacterial pathogens isolated were differ between patients: Most E.coli isolated were sensitive to Gentamicin, Ciprofloxacin and Meropenem, and resistant to Amoxicillin/clavulanate (2:1), Ceftriaxone, nalidixic acid and Ceftazidime. While Klebsiella pneumonia were Sensitive to Gentamicin, Meropenem in addition to sulfamethoxazole- trimethoprim. and resistant to Amoxicilln/clavulanate(2:1) and Ciprofloxacin.
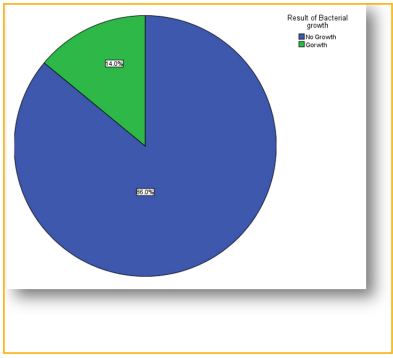
Figure 1: Result of Blood culture
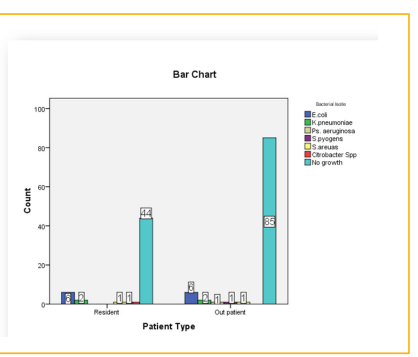
Figure 2: Result of Blood culture VS type of patients.
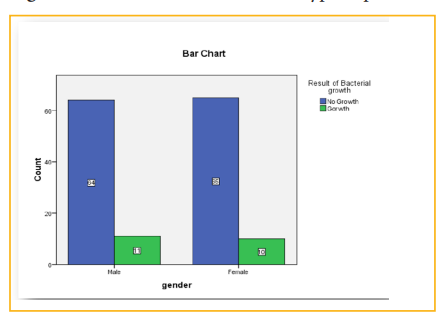
Figure 3: Result of Blood culture according to gender
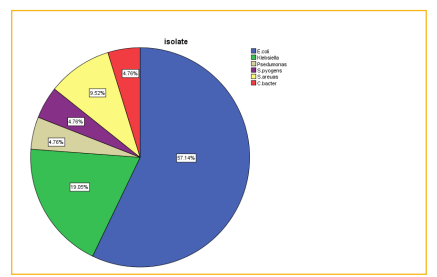
Figure 4: Type of Bacterial isolates.Discussion
In sub Saharan countries including Sudan septicemia is an important cause of illness and death in children, the mortality rate approaches 53% which makes it a significant health problem in developing countries this study is the first comprehensively to address of pathogens causing BSIs in cancer patients from Sudan. E.coli (57.1%) and Klebsiella pneumonia (19%) were found to be the predominant pathogens causing BSIs among Cancer patients in our study setting [11]. and this finding is similar studies conducted previously, the most predominant Gram-negative bacteria isolated from BSIs in patients with cancer were those in the Enterobacteriaceae family including E.coil, K.pneumoniae, and/or P. aeruginosa [12 -15]. However, the latest studies from the UK and Ghana and others from southeast Iran (12.3%), South Africa (24.3%) and Malaysia (23%) showed that CoNS was the predominant Gram-positive pathogen [16-19]. In addition in the past two decades the major changes have been seen in bacteria causing infection in cancer patients. A shift from predominant of gram negative bacteria to gram positive bacteria has been observed. European Organization for Research and Treatment of Cancer (EORTC) is an international organization. The incidence of bacteria in cancer patients has changed considerably over past four decades [20]. All cancer patients in this study received chemotherapy suffering from septicaemia specially those over 50 year of age, this assert that chemotherapy hurts the immune system and cause over growth of bacteria in gastrointestinal tract by providing an alkaline environment in the article of Moran et al [21,22]. Our study was not without limitations. Anaerobic microorganisms were not isolated, as we only used aerobic culture techniques. Since this study used blood samples only, the range of bacterial pathogens to be isolated was limited.