Author(s): Prabudh Goel*, ,Jile Dar Rawat, Piyush Kumar and Sarita Singh
Objective: To describe the ‘Bird-Winged Coronal-Collar Skin re-arrangement modification’ of the Tubularized Incised Plate (TIP) urethroplasty to preserve the inner preputial skin on the ventral surface of the penile shaft.
Material and Method: Study Group: Prospective review of the results of a single surgeon with Bird-Winged Coronal-Collar skin re-arrangement modification of TIP urethroplasty (n=111; mean age 4.9 years) of distal (n=76) and mid-penile (n-35) hypospadias (mean follow-up 37 months).
Control Group: Retrospective review of a single surgeon’s results of distal and mid-penile hypospadias repair with standard TIP urethroplasty (2007-11). Outcome parameters (to compare non-inferiority of the modified technique): Urethro-cutaneous fistula (UCF) at voiding trial and follow-up at 3 months, wound infection, complete dehiscence, local edema, meatal stenosis and quality of urinary stream. Statistical analysis was done with the Fischer Exact Test.
Results: With this technique, the authors could provide an inner preputial cover on the ventral/ ventro-lateral aspects of distal penile shaft in all but one patient (complete dehiscence).The results of ‘bird-winged coronal-collar skin re-arrangement’ modification were not-inferior/ comparable to those of standard TIP urethroplasty.
Conclusions: The modification is technically feasible and reproducible and the overall results of urethroplasty were not inferior to the standard TIPS procedure.
The prepuce is one of the two features (corpora-cavernosa being second) which is common to external genitalia in all primates. The use of prepuce for urethroplasty has been described in a variety of ways including free grafts or pedicled flaps for inlay, onlay or tubularization [1]. Unless preputioplasty is contemplated during hypospadias repair, the prepuce is discarded, in significant part if not whole, in the process of skin rearrangement. Moreover, there is a perennially-ongoing debate about the status of prepuce: should this universal piece of anatomy be regarded as a blessing or is it dangerous and unhealthy [2].
The prepuce is an integral part of external genitalia providing an anatomic cover to the glans penis (males) or clitoris (females). It is a source of skin for the erect penis and assists in smooth movement between the mucosal surfaces during coitus. The unique innervation provides for the erogenous properties. The protopathic sensitivity of the corpuscular receptor-deficient glans penis and the encapsulated receptor-rich preputial-ridge complement each other in generating an erogenous zone [3-5]. The penile dartos within the prepuce consists of smooth muscle richly invested with elastic fibres and is temperature-dependent allowing for volume changes during erection [6]. The inner prepuce contains apocrine glands which secrete cathepsin B, lysozyme (destroys bacterial cell-wall), chymotrypsin, neutrophil elastase, cytokines (pro-immunity) and pheromones (such as androsterone) [7]. With this background, the authors have modified the final skin-arrangement in standard TIP urethroplasty to preserve the inner prepuce skin on the ventral/ ventro-lateral surface of distal penile shaft.
The results of bird-winged coronal-collar skin re-arrangement modification were studied prospectively over four-years (2011- 15) in fresh patients with distal/ mid-penile hypospadias (same surgeon). Out of 157 patients of distal/ mid-penile hypospadiasfollowing patients excluded: redo surgery (n=26), prior circumcision (n=5), chordee without hypospadias (n=2), and surgery by other technique (n=13). One hundred eleven patients finally formed the study group (distal penile=76 and midpenile=35). The age at the time of surgery varied from 1 to 14 years (mean 4.9 years). Follow-up duration varies from 11 months - 4.9 years (mean 37 months).
A retrospective review of a single surgeon’s results of distal and mid-penile hypospadias repair (redo cases excluded) with standard TIP urethroplasty operated over four-years (2007-11) was performed. Data retrieval was possible in 96 of 136 patients satisfying the inclusion criteria.
Non-inferiority comparison parameters included UCF (coronal/ proximal) at first voiding trial and follow-up at 3 months, wound infection, complete dehiscence, local edema, meatal stenosis and quality of urinary stream.
Statistical analysis was done with the Fischer Exact Test using the Easy Fischer Exact Test Calculator at http://www.socscistatistics. com/tests/fisher/Default2.aspx. A p-value<0.05 was considered significant.
[Figure 1A] A stay was taken on the glans with 4-0 silk suture. Urinary bladder was catheterized with an appropriate-sized infant feeding (avoided in the operative-images for better demonstration of surgical steps). Three stay sutures (4-0 silk) were taken at uniform intervals along the border of the dorsal preputial hood. ‘Tennis-racket’ incision was marked as depicted. The curved position of the ‘tennis racket’ was positioned along the junction of the outer and inner prepuce spread out with the help of three stay sutures. The handle of the ‘tennis racket’ was positioned at the lateral border of the urethral plate and the base encircled the meatus of the native urethra.
[Figures 1B-C]Separation of the inner and outer prepuce in
the region of the preputial hood was aided by hydro-dissection
(injection of sterile saline in the plane between the two layers
with a hypodermic needle).
[Figure 1D] Incision was made in the midline proximal to the native
meatus to enter the subdartos plane and the dissection was extended
along the proposed lines. Penile degloving was completed till the
peno-scrotal junction. Ventral tethering lateral to the urethral plate
was excised [Figure 1b]. Gitte’s test was performed to confirm
complete release of chordee. Additional manoeuvres were performed
for chordee correction whenever required.
[Figure 1E]Para-urethral incisions were carried forward onto the glanular ridges and glans wings were raised [Figure 1c]. Urethra proximal to the urethral meatus was slit in the midline proximally whenever found to be hypoplastic or the meatus was stenotic.[Figure 1F] Urethral plate was incised deep down upto the corporal bodies as described by Snodgrass [4]. [Figure 1G] Urethral tubularization was done with vicryl 6-0 continuous suture starting proximally and advancing distally. Glans wings were approximated with vicryl 6-0 interrupted sutures. The laterally splayed dartos already lifted laterally, over-turned onto the neourethra and secured with vircyl 6-0 for additional support. [Figure 1H] Local or penile dartos was mobilized to provide an additional cover to the neo-urethra and secure the suture line.
[Figure M] The inner preputial coronal collar is oriented in a v-shaped configuration and gives the appearance of the spread-out wings of a bird; hence the name of this procedure. [Figure N] The proximal skin tube created by degloving the shaft of the penis was also slit partially in the midline dorsally and used to provide skin cover to the remaining shaft. No preputioplasty was performed in this procedure. The stay over the glans was used to secure the catheter. [Figures O-Q] The final appearance of the penis after completion of urethroplasty is depicted laterally, dorsally and ventrally. A sterile circular cotton-gauge compressive dressing over an antibiotic ointment and paraffin gauge was applied.
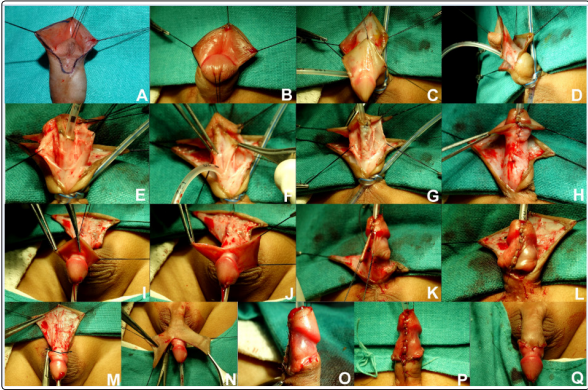
Figure 1: Operative Images for ‘Bird Winged Coronal Collar Modification’ for Tubularized Incised Tip Urethroplasty. For details pertaining to individual images kindly refer to the section on Operative Procedure
Dressing was kept in-situ for four days after surgery.
Patient was given the first voiding trial after removal of catheter (day 10). Quality of stream and presence of any UCF were recorded.
Antibiotic chemoprophylaxis for six weeks and instructions to void voluntarily at frequent (1 hourly) intervals for three weeks after surgery to avoid high voiding pressures. First Follow-up @ two weeks after discharge, monthly thereafter for three months and then three monthly. Voiding trial was repeated.
Local edema was managed with warm compresses. Meatal stenosis was managed with meatal calibration and dilatation. UCF were managed with digital occlusion; presence of meatal stenosis was ruled out by meatal calibration. Fistula closure was attempted only after six months.
With this technique, the authors could provide an inner preputial cover on the ventral/ ventro-lateral distal penile shaft in all but one patient (complete dehiscence). The results of urethroplasty have been tabulated in Table 1.
| Outcome | Control Group n=96 | Study Group n=111 | p value sig <.05 | |
|---|---|---|---|---|
| 1. | Coronal UCF @ voiding trial | 9/96 | 4/111!! | 0.148585 |
| 2. | Other UCF @ voiding trial | 8/96 | 6/111 | 0.42135 |
| 3. | Coronal UCF @ 3 mths. Follow- up | 10/89$$ | 4/111 | 0.04958 |
| 4. | Other UCF @ 3 mths. Follow- up | 9/89$$ | 7/111 | 0.432757 |
| 5. | Cumulative UCF (voiding trial and 3 mths) | 19/89 | 11/111 | 0.028913 |
| 6. | Complete dehiscence | 3/93 | 1/111 | 0.33276 |
| 7. | Wound infection | 6/93 | 7/111@@ | 1 |
| 8. | Meatal stenosis* | Data NA | 23/110 [12 @ first voiding & 11 in follow-up] | NA |
| 9. | Local oedema (>3 weeks) | Data NA | 24/111 | NA |
!!: Of 10 patients in the study-group who presented with a UCF at the time of first voiding, 8 had a good stream while the other 2 had a thin stream from the neo-meatus. The patient who developed UCF after discharge from hospital also had a thin stream. Patients with UCF were put on regular meatal-calibration and digital-occlusion of the UCF. The UCF closed spontaneously in 7 patients (all coronal n=4); three patients were operated after failed trial of conservative management for more than 6 months 1 patient is awaiting fistula closure.
$$: Follow-up @ 3 months was available for 89 of 96 patients (including 17 patients with UCF @first voiding) in control-group; remaining 7 have been excluded from further calculations.
@@: 5 responded to upgrading the oral antibiotic and local application of an antibiotic ointment (fusidic-acid). One patient developed an UCF at the junction of the bird-winged flap and the penile-shaft skin (non-coronal UCF group).
Study-Group -11 of 111 (9.91%) vs Control-Group -19 of 89 (21.34%) (p = 0.028913).
Complete dehiscence: Study-Group-n=1 of 111 (0.90%); infective-etiology. Control Group- n=3 of 93 (3.22%); infectiveetiology (p=0.33276).
Wound Infection: Study-Group: n=6 of 110 and 1 patient with complete dehiscence (7 of 111; 6.31%). Control-Group: n=3 of 93 and 3 patients with complete dehiscence (6 of 93; 6.45%).
Meatal Stenosis: Study Group: n=23; all responded to meatal calibration.
Warm compresses were initiated (n=24) when oedema persisted for more than three weeks.
The prepuce is much more than a mere fold of skin; it is a complex pentalaminar structure formed by the junction of ectoderm, neuroectoderm and mesenchyme in the midline. The combination of preputial folding with ingrowth of cellular lamella leads to the formation of prepuce, glans, corona and the mucosa of the coronal sulcus. This also explains ‘physiological phimosis’; the squamous mucosa of glans penis, coronal sulcus and prepuce are formed in unison [8]. The fused mucosa of the glans and the inner prepuce gradually separate by a spontaneous biological process to form a slit-like space in-between. The five layers consist of the inner squamous epithelium, lamina propria, dartos, dermis and outer skin.
A large variety of nerve endings have been shown to be present in the prepuce: 1) Meissner’s corpuscles which are sensitive to light touch and considered to be the most important in terms of erogenous sensations , 2) Pacinian corpuscles which are sensitive to pressure sensations, 3) Ruffini’s corpuscles or the mechanoreceptors, 4) end-bulbs of Krause which are sensitive to cold, and 5) free nerve endings, sensitive to pain [9-11]. The maximum concentration of nerve endings is seen at the junction of outer and inner prepuce. The inner preputial mucosa can be further sub-divided into smooth and ridged mucosa. The ridged mucosa is that part of the inner prepuce which is situated near the mucocutaneous junction and is like a pleated-band. It contains 10- 12 transverse ridges which are abundant in tactile nerve endings of Meissner (Meissner’s corpuscles) [12].
The vascular supply to the outer prepuce is maintained by the branches from the penile shaft skin (through four branches from the external pudendal arteries) [13]. The vascular supply to the inner preputial skin is maintained from two sources: firstly, from the cross-communicating branches arising from the vessels supplying the outer preputial skin and secondly from the glanular branches. In our technique, the cross-communicating branches are severed during the procedure. However, the glanular branches remain intact and continue to vascularise the bird-wings which are comprised of the inner layer of the preputial hood (the inner preputial skin) which has been separated from the outer prepuce and translocated ventrally to approximate in the midline. The birds-winged flaps are connected to the glans at their base and their height (length along the shaft of the penis measured from their attachment on the corona) is almost half of their width. This is absolutely in coherence with the plastic surgery principles of ‘rotation of vascularised flaps’.
There are two types of primary sensory receptors in the skin: free nerve endings and encapsulated or corpuscular receptors. The free nerve endings are found in most of the skin but the encapsulated receptors are concentrated in regions which are required to have a high touch sensitivity such as the fingertips, lips, perianal skin, transitional areas from skin to mucous membranes and the external genitalia including the prepuce. The significance of the highly specialized and complimentary neuroanatomy of the penile prepuce and the glans in providing a complex sensory platform for normal sexual behaviour can be further derived from the observed trends during the process of evolution [5].
The corpuscular innervation of the human prepuce has become enriched with a concomitant decrease in the density of the same receptors in the human glans as compared to the lower primates [14]. With this background, the authors have tried to preserve a part if not the whole preputial skin while performing urethroplasty in hypospadias patients. A completely skin lined penile shaft may still have free nerve endings but the concentration of encapsulated receptors (find touch) will be relatively scarce. With the ‘birdwinged coronal-collar skin re-arrangement scheme, the dorsolateral inner preputial skin (with specialized touch sensitivity) is transposed ventrally while preserving its blood-supply from the glans penis.
A comparison of the surgical results of the modified techniques with the same surgeons’ previous results were not found to be inferior in any way. In fact, the authors have witnessed a decline in the overall fistula rate. Formation of UCF was observed in 11 of 111(9.91%) in the study group as compared to 19 of 89(21.34%) in the control group. However, the same may be ascribed to reasons other than the modification of the technique such as growing surgical experience and finesse, use of dartos of flap to cover the suture line, finer suture materials and better antibiotics.
The ‘bird-winged coronal-collar skin rearrangement’ modification to the standard TIP urethroplasty is instrumental in preserving the inner prepuce on the distal portion of ventral/ ventro-lateral penileshaft in view of its peculiar neural innervation. The modification is technically feasible and reproducible; the results of urethroplasty are not inferior to the standard TIPS.