Author(s): João Vale *, Sara Diniz , Eva Pereira , Vânia Oliveira and Pedro Cardoso
Synovial sarcoma comprises about 5% to 10% of soft tissue sarcomas. Initial growth is often slow and a small circumscribed tumour may misleadingly appear to a benign lesion by clinical examination and imaging, occurring in up to 50% of cases. The modalities of treatment of foot malignant conditions depend on histological diagnosis and staging. A radical surgical procedure in the distal region of the lower limb is often difficult due to a limited soft-tissue situation and can result in soft-tissue defects. Plastic surgical techniques remain particularly indispensable in the treatment of such distal tumors.
Authors present a hindfoot synovial sarcoma, diagnosed with a incisional biopsy, in which a wide margin surgery was achieved and a limb salvage was permitted by a sural fasciocutaneous flap.
Soft-tissue sarcomas are rare tumours of mesenchymal origin, and are 1% of all adult malignancies. About 60% are located in the extremities [1]. The lower extremities are affected more frequently than the upper extremities, with a ratio of 3:1 [1]. Synovial sarcoma (SS) is a malignant mesenchymal neoplasm with partial epithelial differentiation, that occurs predominantly in older children and young adults and that has been shown to occur at almost any anatomic site, comprising about 5% to 10% of soft tissue sarcomas [2,3]. SS displays a variable degree of epithelial differentiation, including gland formation, and has a specific chromosomal translocation t(X;18)(p11;q11) and that leads to formation of a SS18-SSX fusion gene [3]. The common SS clinical presentation is a painful mass. Initial growth is often slow and a small circumscribed tumor may misleadingly appear to a benign lesion by clinical examination and imaging. It occurs mainly in para-articular regions close to joint capsules, although occurrence within a joint is very rare [3,4]. The modalities of treatment of foot malignant conditions depend on histological diagnosis and staging. Different treatment options should be discussed in an multidisciplinary meeting, in a specialized referral center. [5, 6].
Limb-sparing surgery with a wide margin is generally preferred because it can achieve a low rate of local recurrence with an acceptable level of morbidity [7].
A radical surgical procedure in the distal region of the limb is often difficult due to a limited soft-tissue situation. Attainment of clear margins becomes much more difficult in tumour of extremities and can result in soft-tissue defects. Plastic surgical techniques remain particularly indispensable in the treatment of such distal tumors, and in the foot and ankle area are required in about 50% of cases and are associated with a high success rate [1]. Authors present a hindfoot synovial sarcoma in which a wide margin surgery was achieved and a limb salvage was permitted by a sural fasciocutaneous flap.
A 45-year-old male, presented a 9 months history of painful mass on the lateral side of the hindfoot. MRI showed a solid tumour in subcutaneous cellular tissue in the lateral and plantar slope of the heel body, measuring about 15x25x9mm, with slightly irregular contours (shown in Figure 1). A surgical incisional biopsy was made an it was establish a monofasic grade 3 SS. Staging was performed with thoraco-abdomino-pelvic CT, with no evidence of secondary disease.
Due localization in subcutaneous cellular tissue in the lateral and plantar slope of the heel body, it was necessary to remove part of the adjacent skin, creating a important skin defect. To ensure free margins, a part of adjacent cortical bone of calcaneus was removed as well (shown in Figure 2). To cover the skin defect a sural fasciocutaneous flap was performed. (shown in Figure 2). Seven days after this intervention, a partial-thickness skin-graft of the homolateral thigh covered the donor area (shown in Figure 2).

Figure 1: MRI showing a densification area of subcutaneous cellular tissue in the lateral and plantar slope of the heel body, measuring about 15x25x9 mm, with slightly irregular contours, with hypo signal areas, raising suspicion of synovial sarcoma
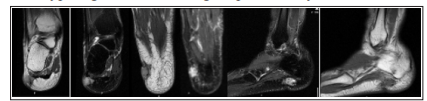
Figure 2: A, B, C, D and E: Wide resection followed by skin defect reconstruction with sural fasciocutaneous flap. F: partialthickness skin-graft of the homolateral thigh covered the donor area after 7 days. G: graft and flap evolution at 1 month; H: clinical appearance one year after surgery
Histologic report confirmed a monophasic synovial sarcoma, resected with wide margins, rpT1 Nx R0.
One month after surgery the patient was submitted to adjuvant RT in the right calcaneus.
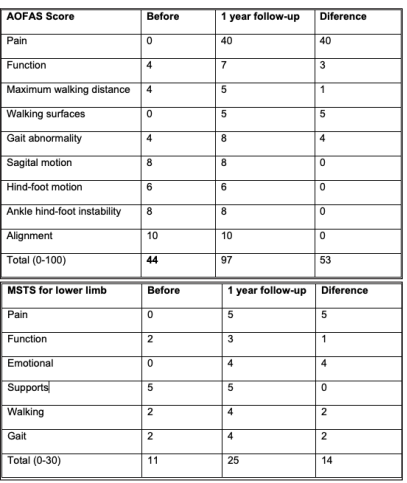
One year after surgery he presents complete range of motion and an improvement from 42 to 97 in a total of 100 in American Orthopedic Foot & Ankle Society (AOFAS) score and 11 to 25 in a total of 30 in Musculoskeletal Tumor Society (MTSS) scoring system (Table 1 and 2).
There is no evidence of recurrence or secondary disease during follow-up until now.
The classic local treatment of malignant conditions of the foot and ankle was below-knee amputation at different levels, due to complex foot anatomy [5, 8]. Nowadays, with the development of adjuvant therapies, some patients may benefit from conservative surgery or partial amputation [5]. The recommended surgery for soft-tissue sarcomas is wide resection, intending to provide tumour free margins [5,7]. The surgeon should remember that the primary goal of surgery is the oncological result. If complete resection is compromised with a high risk of local recurrence amputation is advised [5].
Cribb et al. retrospectively investigated the oncological and functional outcome of 27 patients who had limb-sparing surgery for a soft tissue sarcoma of the foot or ankle and reported that all surviving patients were able to wear normal shoes and none required a walking aid [9]. Foot can be divided into four major areas based on different requirements for reconstruction and the types of flaps available: proximal and distal weight-bearing plantar areas, the dorsum, and the ankle region that includes the malleoli, the Achilles tendon, and the non-weight-bearing heel area [1].
Margins to adjacent functional structures (fascia, synovia, periosteum, and perivascular and perineural tissue) should be taken into account in the oncosurgical considerations [1]. SS is an aggressive sarcoma, and an en-block resection was necessary, resulting in a 3x3 cm cutaneous defect in proximal plantar area.
Proximal plantar area is difficult to treat, because it is a thick, loadcapable, and stress-resistant skin, and donor regions do not meet the requirements with regard to tissue quality and functional needs [1]. Defects larger than 3 cm2, without bone involvement, need to be covered by free fasciocutaneous, free musculocutaneus flap or local flaps to ensure a durable soft-tissue coverage preventing recurrent ulcerations, improving the scar qualities and reducing strains on the scars [1].
Authors chose a sural fasciocutaneous flap which present some advantages: acceptable skin defect coverage and adequate padding of bone structures. In contrast to free flaps, local flaps do not require intensive postoperative flap inspections, postoperative positioning protocols and anticoagulation regimens are less stringent [1].
This case shows that reconstructive plastic surgery can play an important role in preservation and reconstruction of function after the resection of foot malignant tumours. Knowledge of plastic reconstructive surgery techniques and its proper use can improve the quality of life of the oncologic patient.
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
The authors have no conflicts of interest to declare.