Author(s): Chowdhury Md Navim Kabir
Renal impairment is one of the severe non communicable disease around the world. Especially patients of diagnosed/newly diagnosed renal impairment those who needed surgery are more focused for preoperative and postoperative preparation. Serum creatinine is the prime biochemical marker for assessing renal function and level of impairment is widely measured by this marker as well as Glomerular Filtration Rate (GFR).
Objective: Factors responsible for serum creatinine fluctuation in preoperative and postoperative period and its minimizing process the ultimate goal of this study.
Method: 37 patients were participated in this cross-sectional study who were being previously diagnosed/newly diagnosed. They were admitted in different tertiary level hospitals for emergency or elective surgery.15 patients were admitted in renal function impairment stage, 22 were admitted as normal patients. Values of creatinine at pre admission stage and 2nd/3rd post admission follow up were compared.
Results: 0.41 was the average of 22 patients’ creatinine between pre admission and 2nd/3rd follow up. The responsible factor like prolonged staying, immobilization, co-morbidities, different preoperative antibiotics, NSAIDs were also inducer for creatinine elevation. After postoperative hemodialysis rapid decrease of creatinine seen on normal patients but this decrease very much minor on CKD diagnosed patients.
Chronic Kidney Disease (CKD) is a common systemic in the world. Due to lack of balanced diet along with unhealthy life style and routine body checkup many persons become victim of this disease Worldwide over 800 million of people are the victim of this disease. These patients needed persistent monitoring like renal friendly drugs dosage, dietary habits and lifestyles modification. In operative procedure they needed intensive preparation either emergency or elective. However, cardiological, hematological assessment routinely done under the supervision of surgeon, anesthesiologist with direct consultation of nephrologist. Besides these systemic monitoring, serum creatinine are the prime investigation for assessing kidney function. Satisfactory creatinine level in serum can be a lifeline for surgeon and especially for patient’s point of view those who are being immobilized for a long time. For this purpose value of serum creatinine is vital for preoperative and postoperative purpose and fluctuation of this be a obstacles for patient’s sound preoperative and postoperative preparation.
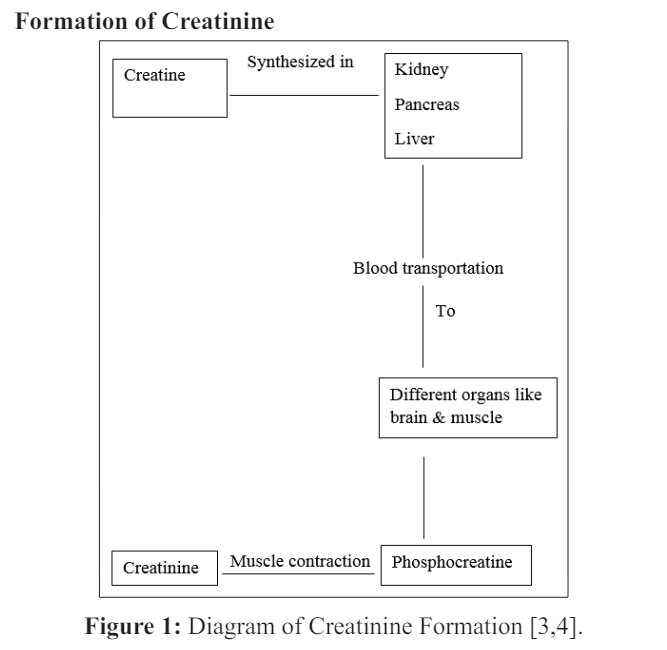
Creatinine is a chemically waste product formed by break down of creatine. It is transported through bloodstream to the kidneys and washed out. Its production dependent on muscle mass and lean muscle mass of a human is directly proportionate to the amount of creatinine in blood. Creatinine is diet independent so its concentration depends on the rate at creatinine excreted through the both kidneys [1-2].
In general thoughts, elevation of serum creatinine usually in the patients of renal function impairment. But in different cases level of creatinine can be fluctuated. Normal range of creatinine on healthy males 07-1.4 mg/dl and 06-1.3 in healthy females. Amount of creatinine can be raised or decreased due to physiological or pathological body conditions. It can be reversible after spontaneous resolution of the underlying condition. Body fluid or electrolytic imbalance can be responsible for this. In acute loose motion, massive fluid loss along with vital minerals. If dehydration state cannot be corrected it may be responsible for acute renal impairment with creatinine elevation. In most of the cases underlying loose motion resolution reverse the kidney function to the normal state. But in some cases hemodialysis or peritoneal dialysis may be indicated if spontaneous resolution doesn’t occurred. As amount of creatinine is directly related to the muscle bulk, any types of malnutrition may be reduced serum creatinine. In pregnancy period, reduction of creatinine is occurred which physiologically reversed after delivery. Serum creatinine may be fluctuated due to various causes in preoperative and postoperative period. It can be happened in both old/newly CKD diagnosed patient or patients of normal renal function. Hydration state, history of high protein diet, long time immobilization history also play vital role in creatinine fluctuation in preoperative and postoperative period. Without systemic emergency and deterioration probability, surgeons and anesthesiologists don’t prefer operative procedure. History of hemodialysis/peritoneal dialysis is also a factor for creatinine fluctuation [5-7].
Total 37 participants with age range of 33-67 years participated in this cross sectional study those who have history of creatinine fluctuation in preoperative/postoperative period during their admission in different tertiary hospitals. 22 of them were male and 15 of them were female. Out of 22 male participants, 9 were previously CKD diagnosed and 5 of them took hemodialysis in every week. Out of 15 females, 6 were previously CKD diagnosed and 2 of them had history hemodialysis. Out of 22 normal males and females participants, 10 patients who had previous documented evidence of serum creatinine within normal range, sudden rise of creatinine after hospital admission. Out of these 10 patients, 6 were admitted with immobilization history due to road traffic accidents and 4 of them had postoperative complication history. The most important findings that they had at least one comorbidities (Diabetes Mellitus/hypertension/dyslipidemia) [8-10].
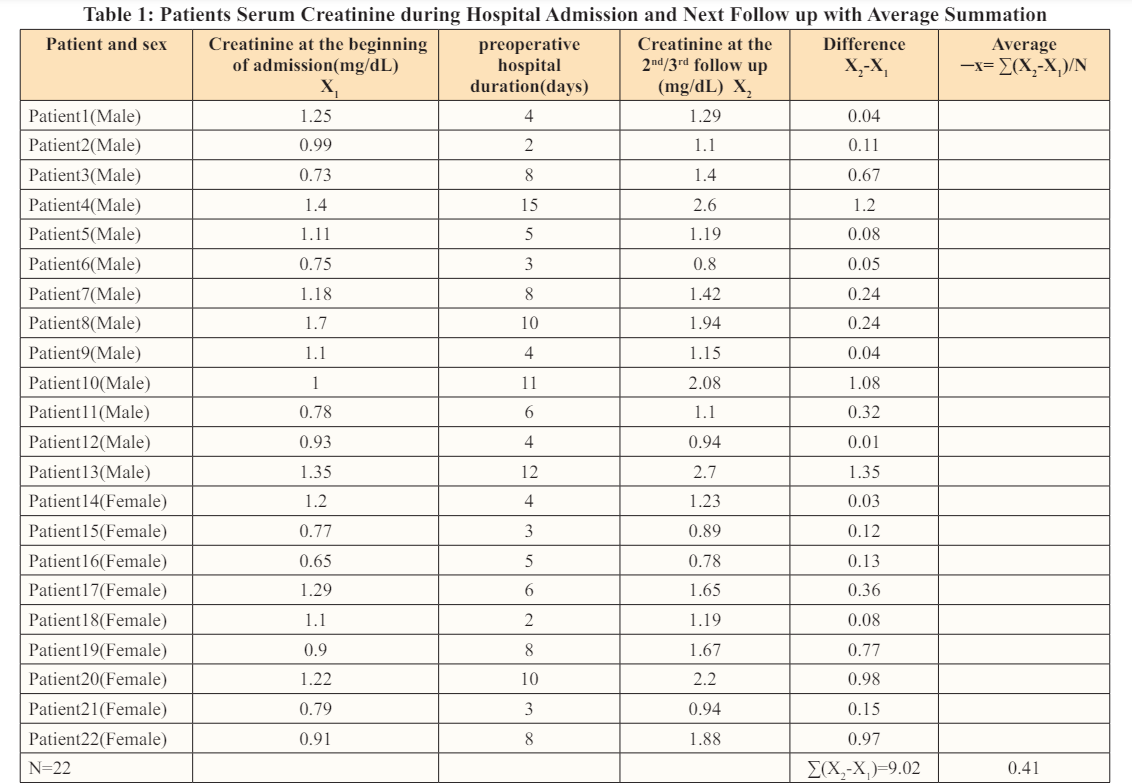
In table 01, data of 22 patients those who had not documented clinical symptoms of renal impairment and normal serum creatinine have showed. Their serum creatinine during hospital admission and next (2 nd /3 rd follow up) with hospital duration up to surgery are highlighted. Out of the 22 patients, 4 males and a female need to be hospitalized 10 days or more than 10 days. Out of the 4 males lowest creatinine value during admission time was 1mg/dL and highest 1.7 mg/dL.1.35 mg/dL is the highest difference between two creatinine sample of these 4 male patients. Average preoperative hospital admission period are 6 days with 0.41 average difference of creatinine values in both follow up [11-15].
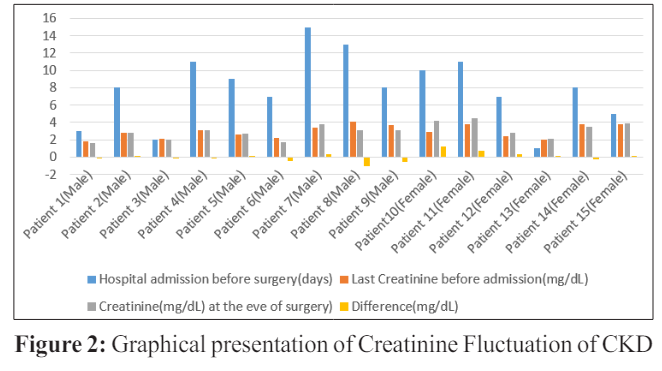
From Table 1 and figure 2 creatinine fluctuation scenario is highlighted. In figure 2, 15 patients those were previously diagnosed as CKD. Out of 15 patients, 9 were male and 6 were female.5 male patients were documented hemodialysis taker and 4 weren’t. Out of these 9 patients, 3 of them needed to be hospitalized more than 10 days and their serum creatinine at the admission was 3.15,3.4 and 4.01 mg/dL respectively. For preoperative fitness purpose and immobilization avoidance they need dialysis. The first and third patient’s follow up creatinine at the eve of surgery were 3.09 and 3.08 mg/dL. These two patients were given hemodialysis and rest of refused. These 3 patients were more highlighted due to their prolonged hospital staying period because of fitness and post traumatic stability. In comparison, patients those who were no history of renal impairment ahead in fluctuation with patients those who were CKD diagnosed. Average creatinine difference of normal patients was 0.41 and 0.02 was average for impairment patients [16-19].
Patients those who had high serum creatinine value at the eve of surgery and difference along with prolonged hospital admission staying were given importance specially their postoperative creatinine value as well as postoperative events.
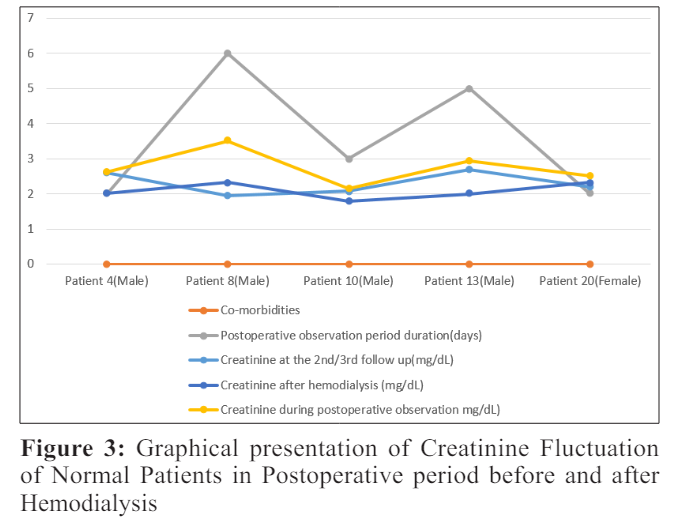
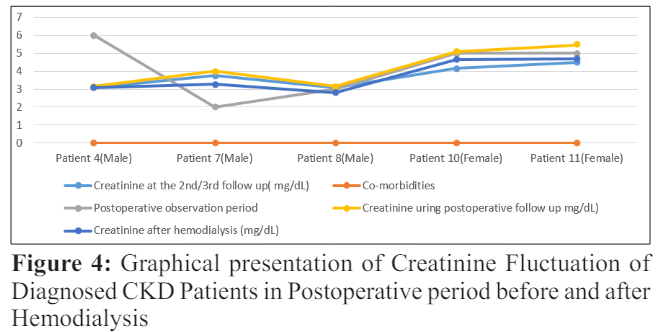
Figure 3 and 4 highlights 37 participant’s serum creatinine fluctuation after surgery. Serum creatinine changing during postoperative period as well as impacting factors also being highlighted. In figure 3, 22 patients those who had no previous history of renal impairment were being admitted for operative purpose, their fluctuation of creatinine before and after dialysis were being focused. Also impact of comorbidities on this fluctuation being emphasized. Patient having both DM (Diabetes Mellitus) and HTN (Hypertension) were needed to be more postoperative hospitalization than single comorbid patient. Also raising of creatinine mentioned with these multi comorbid patients. Average fluctuation of creatinine here-0.658 mg/dL. On the other hand, figure 4 emphasis the remaining 15 patient’s creatinine those who had history of renal impairment associated with multiple comorbidities. Chiefly DM and HTN had seen as comorbidities in the patients who needed prolonged postoperative staying(maximum 6 days).Maximum 5.47 mg/dL is the highest postoperative serum creatinine value and 3.15mg/dL is the lowest. Average differential value between pre hemodialysis and post hemodialysis creatinine is -0.618 mg/dL [20-24].
Increasing serum creatinine during postoperative period was triggered by some factors. Specially prolonged preoperative staying, comorbidities, medications in order were responsible for fluctuation.
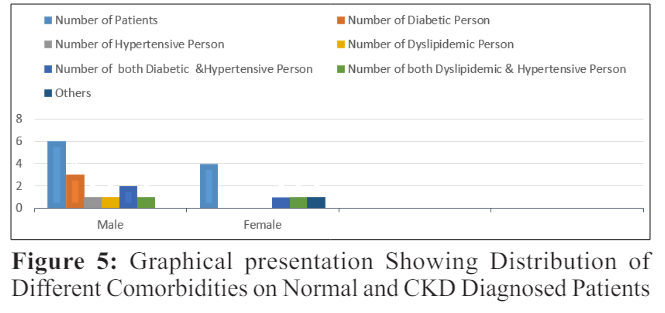
From figure 5 distribution of comorbidities among patients has been emphasized. Prevalence of diabetes, hypertension and dyslipidemia being showed among the patients. Individually 3 male patients having diabetes, 1 male had hypertension.3 patients had both diabetes and hypertension where 2 were male and rest of female. These 3 patients had history of prolonged post observation period which may be responsible for rising creatinine. It is also applicable for patients with hypertension and dyslipidemia due to their 5 days postoperative duration. [25-27].
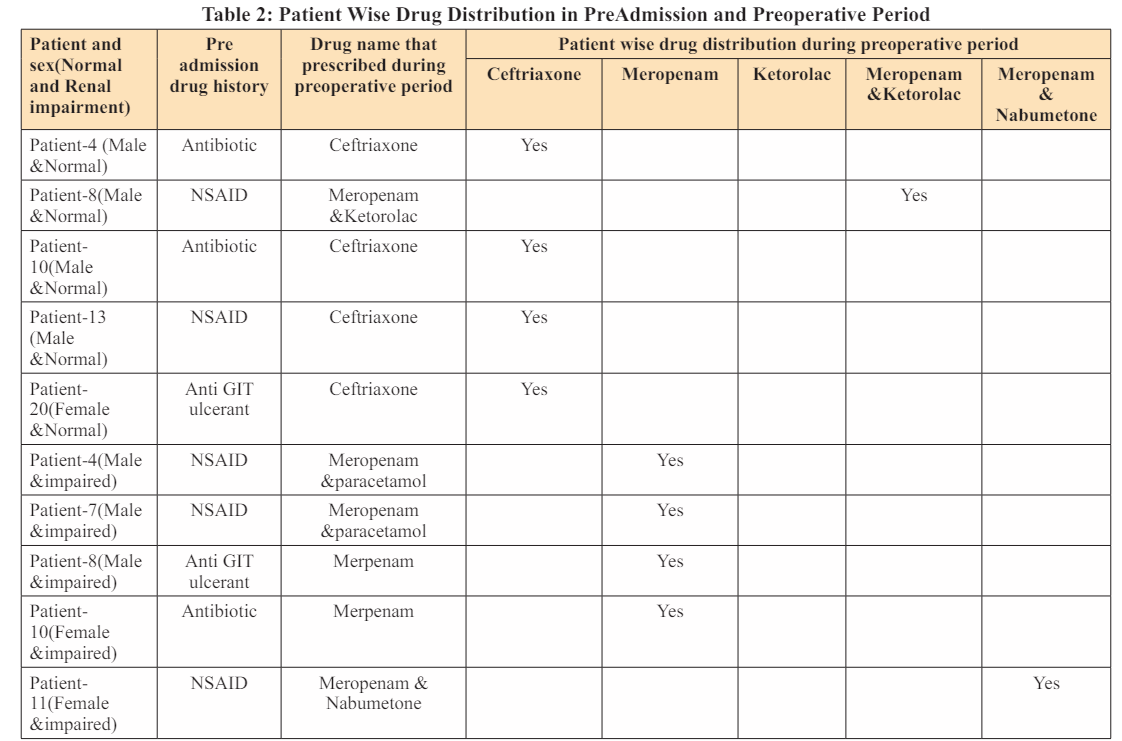
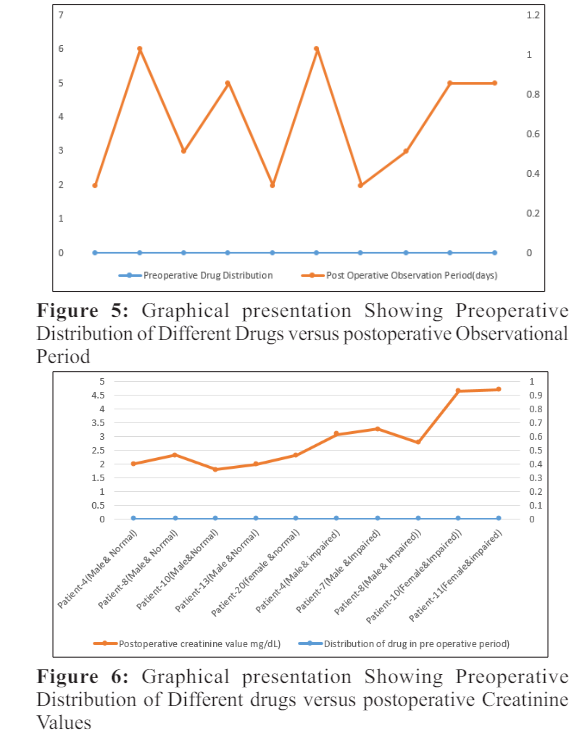
From table 2, figure 5 and 6 shows the graphical relationship among prescribe drugs history (preoperative and postoperative period) postoperative admission period and effect upon creatine. Ceftriaxone, meropenam, ketorolac, nabumetone are the drugs that were being prescribed before admission and preoperative hospital admission. Patients those who weren’t documented having any kind of renal impairment are typically prescribed ceftriaxone and ketorolac(for relieving pain in road traffic trauma),serum creatinine were increased with prolonged hospital duration.CKD patients were given meropenam ,paracetamol for relieving symptoms. Due to peroperative anesthetic drugs and muscle relaxants, creatine were increased bur after hemodialysis creatinine decreased. In normal patients fluctuations were more than the patients who were given dialysis as well as diagnosed as CKD [28].
Total 37 patients were participated in this cross-sectional study where 22 patients who hadn’t no history of kidney diseases On the other hand, rest of the 15 patients were documented as CKD patients and 7 of them had history of hemodialysis. These patients were admitted tertiary level hospitals for surgery purpose. As base line investigations, serum creatinine compared with pre admission stage and 2nd/3rd follow up. Average value of creatinine of 22 normal patients were 0.41. The important finding was elevation of creatinine after prolonged hospital staying.10 patients needed to be stay 10 or more than 10 days. Reasons like preoperative elevation of creatinine, post road traffic accident induced immobilization triggered that elevation process. Patients comorbidity history also been focused during survey. Diabetes, hypertension, dyslipidemia were the main non communicable diseases were responsible for immunosuppression and creatinine elevation. Males were more prone to diabetes and females were dyslipidemia. Those who had more than one diseases were very much prone to develop kidney diseases. Besides these pre admission drug history as well as after admission different drugs were also been inducer of creatinine elevation. The 10 patients who had prolonged hospital staying history were also habituated in taking antibiotics, NSAIDs in different occasions with/without indications. After admission Ceftriaxone, ketorolac were also triggering creatinine elevation. Per operative muscle relaxants with anesthetic drugs were also responsible. Postoperative hemodialysis helped mostly for stable kidney function by rapid reversing the creatinine value. But this fluctuation were very minor who were in advanced kidney function impairment stage [29-31].
Serum creatinine itself a gold standard biochemical investigation for assessing renal function. The significance of kidney in blood pressure management as well as buffer system maintenance, creatinine focus gross renal stability. For different circumstances elevation and falling of creatinine can be occurred which can be assessed by creatinine without delay. For ensuring uneventful per and postoperative period creatinine fluctuation and its inducer events should be properly monitored for rational medical practice.
The author has no conflict of interest to be declared.