Author(s): Alpaslan Gunduz* and Hasan Ayberk Altug
Bisphosphonates are a class of drugs extensively used in the management of numerous conditions. In patients with bisphosphonate-related osteonecrosis of the jaws, surgical interventions on bone tissue often exacerbate the condition. Alternative treatment methods, including laser and ozone therapies, are being explored to mitigate the adverse effects of bisphosphonates.
Our study was a prospective, randomized, and controlled trial. Total of 80 female Wistar rats were utilized in the study. The animals were divided into five groups. Rats were measured for intravenous zoledronic acid administration. Histopathological evaluations were conducted to assess new bone formation and inflammation intensity within the extraction sockets.
While there is a statistically significant difference between the groups regarding ossification rates on the 7th day, there is no statistically significant difference between the groups on the 14th day. At the end of the seventh day, no statistically significant difference in inflammation scores. At the end of the 14th day, there was a statistically significant difference between the groups regarding inflammation scores.
These findings suggest that laser and ozone therapies enhance new bone formation over the long term and mitigate the adverse effects of bisphosphonates in rats.
In contemporary dentistry, the primary goal across all disciplines is to preserve natural teeth within the jaws. However, tooth and surrounding tissue loss becomes inevitable in certain conditions, such as trauma, systemic diseases, or neoplasms. Prosthetic approaches are employed in such cases, though they require a robust foundation for optimal adaptation. Thus, ensuring the continuity of existing hard and soft tissues remains a critical objective [1].
Teeth and their supporting tissues function in harmonious integration. The loss of teeth, regardless of the cause, is often followed by a gradual loss of surrounding tissues. Most bone resorption occurs within the first year following tooth extraction. Various factors, including systemic diseases, smoking, nutritional status, and pharmacological therapies, influence the health of the remaining bone tissuec [2,3].
Bisphosphonates are a class of drugs extensively used in the management of numerous conditions. However, long-term administration, mainly through intravenous routes, can have adverse effects, including necrotic regions in the jaws and soft tissue exposure due to the impact on bone tissue. Despite their therapeutic benefits, these complications significantly reduce the quality of life [4,5].
In patients with bisphosphonate-related osteonecrosis of the jaws, surgical interventions on bone tissue often exacerbate the condition. Alternative treatment methods, including laser and ozone therapies, are being explored to mitigate the adverse effects of bisphosphonates [6].
Lasers are widely used in various branches of dentistry. In oral and maxillofacial surgery, they exhibit diverse effects on hard and soft tissues. Low-Level Laser Therapy (LLLT) is mainly utilized during the healing phase. Its mechanism of action involves the absorption of specific wavelengths of visible and infrared light by cellular photoreceptors, which transmit the energy to mitochondria. This energy enhancement activates fibroblasts and other cells integral to tissue repair, stimulating the healing process. In recent years, laser biostimulation has been increasingly combined with regenerative methods to enhance the healing of bone defects [7].
Ozone Therapy (OT) is another method that facilitates hard and soft tissue healing and is recognized for its potent antimicrobial properties. OT has been used in treating infectious diseases and oral surgery to promote hemostasis, oxygenation, and infection prevention following osteotomy. It enhances the concentration of red blood cells and hemoglobin while stimulating the phagocytic system. These effects are particularly evident in the capillary-rich regions of the mandible and maxilla. Ozone also aids healing by stimulating biological reactions and the metabolism of calcium, phosphorus, and iron [8].
This study aimed to evaluate the histomorphometric effects of laser and ozone therapies on the formation of new bone tissue in extraction sites of rats treated with zoledronic acid, a bisphosphonate known to affect bone metabolism.
Our study was a prospective, randomized, and controlled trial. Ethical approval was obtained from the Gülhane Military Medical Academy (GATA) Animal Experiments Ethics Committee under decision number 15/42, dated April 10, 2015. The project was registered and financially supported under the GATA directive AR-2015/17, dated November 27, 2015.
Total of 80 female Wistar rats weighing between 200 and 300 grams were utilized in the study. The number of rats in the experimental and control groups was determined through power analysis. The animals were divided into five groups:
Each group was further subdivided into two subgroups for sacrifice on the 7th and 14th days, with eight rats planned per subgroup. Sixteen animals were lost at various stages, and the study was completed with 64 rats.
Eighty 12-week-old female Wistar rats weighing 200–300 grams were randomly assigned to stainless steel cages in eight groups, matching their respective study groups. The animals were housed in controlled environments with 30–70% humidity levels and subjected to a 12-hour light/12-hour dark cycle at 20±2°C. They were fed standard chow and water. The cages and room were cleaned weekly. The rats were acclimated to their new environment for one week before the study commenced.
The weights of 64 rats in the experimental groups (BC, BL, BO, BLO) were measured for intravenous zoledronic acid administration. Their weights were monitored weekly for six weeks to calculate the appropriate dose, administered via the tail vein at 0.04 mg/kg. The control group received intravenously 0.1 ml of isotonic saline for the same duration as the experimental groups.
The weights of 64 rats in the experimental groups (BC, BL, BO, BLO) were measured for intravenous zoledronic acid administration. Their weights were monitored weekly for six weeks to calculate the appropriate dose, administered via the tail vein at 0.04 mg/kg. The control group received 0.1 ml of isotonic saline intravenously for the same duration as the experimental groups [9].
Rats in the bisphosphonate-laser group (BL) received laser treatment every three days, starting on the extraction day. Using the Biolase Epic 10 laser device, a 5-second application was administered at a 5 mm distance. The cumulative effects of the laser guided the specific parameters. These rats were sacrificed on the 7th and 14th days [10].
Bisphosphonate-ozone group (BO) rats were administered ozone gas generated by the Longevity Ozone Generator EXT50 device at 0.7 mg/kg intraperitoneally every two days, starting on the extraction day. The combined bisphosphonate-laser-ozone group (BLO) received treatments identical in dose and schedule to those of the BL and BO groups. Sacrifices were performed on the 7th and 14th days [11].
Histological Assessment and Preparation of Sections Following sacrifice, samples were fixed in 10% buffered formalin for 24–72 hours, decalcified in 10% formic acid with bi-daily changes for one week, washed overnight, and embedded in paraffin blocks after routine tissue processing. Sagittal sections of 4–5 µm thickness were prepared for hematoxylin-eosin (H&E) staining. Sections were deparaffinized at 65°C for one hour, immersed in xylene and alcohol, rinsed in tap water, and stained. Histopathological evaluations were conducted using a Leica DM 4000 B microscope to assess new bone formation and inflammation intensity within the extraction sockets.
New bone formation was quantified using a semi-quantitative method, with the proportion of connective tissue to new bone calculated across the socket at X10 magnification. Masson’s trichrome staining distinguished collagenized structures, aiding in assessing connective tissue and new bone. Microorganisms, including Actinomyces and gram-positive/negative bacteria, were identified via Light Green Periodic Acid-Schiff staining.
Inflammation intensity was scored as follows [4] 0: No inflammation.
1: Mild inflammation.
2: Moderate inflammation.
3: Severe inflammation, abscess, or necrosis.
Data were analyzed using SPSS version 20 (Chicago, IL). The Shapiro-Wilk test assessed the normality of variable distribution. Statistical significance was set at p<0.05. The Kruskal-Wallis H test examined intergroup differences, with post-hoc multiple comparisons identifying specific group differences. Wilcoxon tests were employed for paired variable analysis when standard distribution criteria were unmet. Results with p<0.05 were considered statistically significant, while p>0.05 indicated no significant difference.
The statistical distribution of ossification rates between groups during two different sacrification periods is given in the table (Table 1 % Graph 1). While there is a statistically significant difference between the groups regarding ossification rates on the 7th day, there is no statistically significant difference between the groups on the 14th day.
|
|
Group |
Kruskal Wallis H Testi |
||||||||
|
n |
Mean |
Median |
Min |
Max |
ss |
Rank Avg. |
H |
p |
||
|
Ossification rate on day 7 (%) |
C |
6 |
26,38 |
30 |
3,75 |
35 |
11,41 |
23,67 |
9,5 |
0,04 |
|
BC |
6 |
20,96 |
22,25 |
16,25 |
22,5 |
2,5 |
20,25 |
|||
|
BL |
7 |
10,71 |
7,5 |
5 |
31,2 |
9,19 |
10,07 |
|||
|
BLO |
6 |
12,29 |
11,25 |
1,25 |
25 |
7,96 |
13,17 |
|||
|
Total |
31 |
16,56 |
16,25 |
0 |
35 |
10,27 |
|
|
|
|
|
Ossification rate on day 14 (%) |
C |
6 |
53,25 |
50 |
42 |
75 |
12,9 |
20,83 |
3,1 |
0,53 |
|
BC |
6 |
52 |
54,75 |
41,25 |
60 |
8,31 |
21 |
|||
|
BL |
7 |
42,68 |
45 |
25 |
52,5 |
8,61 |
14,57 |
|||
|
BO |
7 |
44,04 |
45 |
18,75 |
75 |
18,25 |
14,93 |
|||
|
BLO |
7 |
46,25 |
45 |
36,25 |
65 |
9,76 |
14,79 |
|||
|
Total |
33 |
47,34 |
45 |
18,75 |
75 |
12,21 |
|
|||
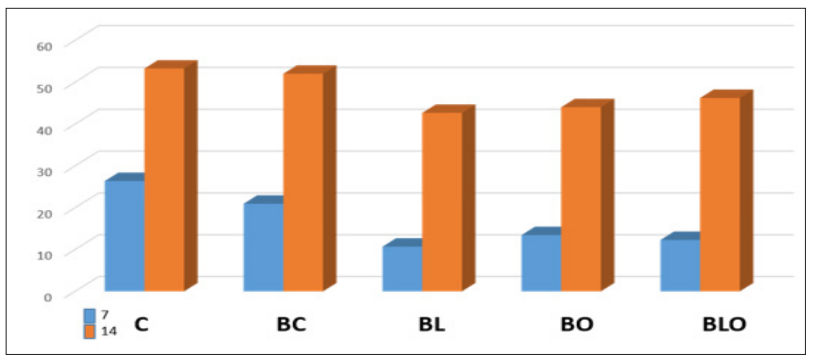
Figure 1: Distribution of Ossification Rates According to Groups.
At the end of the seventh day, no statistically significant difference in inflammation scores was found between the groups. However, the scores of the C, BC, and BLO groups were higher than the others (Table 2, Graph 2). At the end of the 14th day, there was a statistically significant difference between the groups regarding inflammation scores. The 14th-day inflammation score of the C group was significantly lower than the BO group (Table 2).
|
|
Group |
Kruskal Wallis H Testi |
||||||||
|
n |
Mean |
Median |
Min |
Max |
ss |
Rank Avg. |
H |
p |
||
|
Inflammation Scores on Day 7 (%) |
C |
6 |
2,5 |
2,5 |
2 |
3 |
0,55 |
17 |
4,267 |
0,371 |
|
BC |
6 |
2,5 |
3 |
1 |
3 |
0,84 |
18 |
|||
|
BL |
7 |
1,86 |
2 |
1 |
3 |
0,69 |
10,36 |
|||
|
BO |
6 |
2,33 |
3 |
0 |
3 |
1,21 |
17,58 |
|||
|
BLO |
6 |
2,5 |
3 |
1 |
3 |
0,84 |
18 |
|||
|
Total |
31 |
2,32 |
3 |
0 |
3 |
0,83 |
|
|
|
|
|
Inflammation Scores on Day 14 (%) |
C |
6 |
0,67 |
1 |
0 |
1 |
0,52 |
7,67 |
13,974 |
0,007 |
|
BC |
6 |
2 |
2 |
1 |
3 |
1,1 |
18,75 |
|||
|
BL |
7 |
2,14 |
3 |
0 |
3 |
1,21 |
19,93 |
|||
|
BO |
7 |
2,71 |
3 |
1 |
3 |
0,76 |
24,64 |
|||
|
BLO |
7 |
1,29 |
1 |
1 |
2 |
0,49 |
12,93 |
|
||
|
Total |
33 |
1,79 |
1 |
0 |
3 |
1,08 |
|
|||

Figure 2: Distribution of Inflammation Scores According to Groups.
Based on the data obtained from our experimental study evaluating the effects of ozone and laser therapy on the wound area following tooth extraction in rats treated with zoledronic acid, it is concluded that laser and ozone therapies constitute suitable models for assessing experimental new bone formation in rats treated with bisphosphonates. Upon examining the morphology of rat teeth, incisor teeth were preferred due to the sufficient presence of bone tissue in the socket, which is crucial for histomorphometric analysis post-extraction. Although the morphology of the upper incisors posed challenges during extraction, they were selected for this study owing to their accessibility during both the extraction and laser therapy application processes [12].
Significant differences in bone formation rates among the groups were observed on the 7th day. The bone formation rate in the BL group was significantly lower compared to the C and BC groups, and the rate in the BLO group was significantly lower compared to the C group. In all groups, bone formation rates on the 7th day were significantly lower than those on the 14th day. Regarding inflammation scores on the 7th day, no statistically significant differences were observed between the groups (p > 0.05). However, statistically significant differences were noted in inflammation scores among the groups on the 14th day.
In oral, dental, and maxillofacial surgery, improving bone healing and promoting new bone formation, particularly after tooth loss, is influenced by various factors. Bone tissue metabolism is affected positively or negatively by numerous variables, including age, gender, hormones, habits such as smoking, systemic diseases, and medications used by individuals [13,14].
Among these factors, using antiresorptive drugs, which significantly influence bone metabolism, becomes particularly important when considering the remodeling rate of the jawbones. In our study, we aimed to investigate the adverse effects of bisphosphonate-class drugs, specifically intravenously administered zoledronic acid, on bone tissue and explore strategies to mitigate these effects [15,16].
To minimize such adverse effects, various materials and methods, such as laser, ultrasound, hyperbaric oxygen, ozone, growth factors, and blood-derived products (e.g., platelet-rich plasma and platelet-rich fibrin), can be employed to stimulate new bone formation and healing. In this study, we focused on evaluating the potential positive or negative effects of laser and ozone therapies on bone healing [17,18].
Bone tissue is constantly remodeling due to structural stress and the body’s calcium demands. Bone healing is a complex process involving the recurrence of specific stages of skeletal development and growth under the influence of cells, growth factors, and the extracellular matrix [19]. The healing of extraction wounds shares similarities with fracture healing. Immediately after extraction, the alveolus fills with blood, and red blood cells aggregate and settle. As fibrin networks form, blood vessels in the periodontal membrane constrict. If the alveolus does not fill with blood within the first few hours post-extraction, wound healing may be delayed or even fail partially. The blood filling the alveolus also aids in clearing debris from the socket [20].
Amler et al. demonstrated that, following tooth extraction, the socket is initially filled with a blood clot, which is replaced by granulation tissue after seven days. By the 20th day, granulation tissue is substituted with collagen, and new bone formation begins at the base and periphery of the socket. At five weeks post- extraction, two-thirds of the socket is filled with bone. Complete epithelial coverage of the extraction socket requires 24 days, although in some cases, this process may extend to 35 days. The epithelium continuously advances, encapsulating granulation tissue, debris, and small bone fragments. Concurrently, new bone formation begins within the socket, initially at the base and walls, and eventually progresses to the central and apical regions [21].
Devlin et al., in a study involving the extraction of molars in rats, observed remnants of the periodontal ligament during the first two days post-extraction. These remnants became indistinguishable following the invasion of fibroblasts and blood vessels from surrounding tissues. By the fourth day, as spongy bone began to fill the extraction socket, collagen within the remnants of the periodontal ligament became obscured. They reported that after the resorption of alveolar bone, the collagen fibrils within the socket served as a framework for newly forming bone tissue [22].
In a histological study examining the healing of extraction sockets, Pinto et al. reported that, in the control group, the socket was nearly entirely filled with a blood clot by the third day, containing numerous macrophages. By the seventh day, the socket was predominantly filled with newly formed connective tissue rich in fibroblasts. On the 15th day, newly forming bone trabeculae were observed, and by the 28th day, the alveolar socket was filled with thick, well-defined trabecular bone [23].
Magro-Ernica et al., in a histological study on rat extraction sockets, found that by the seventh day, the socket was partially filled with newly formed connective tissue, blood clots, and bone trabeculae located in the apical third. By the 21st day, thick bone trabeculae and mature connective tissue were present in certain areas. By the 28th day, the alveolus was completely filled with mature bone trabeculae [24].
These findings suggest that laser and ozone therapies enhance new bone formation over the long term and mitigate the adverse effects of bisphosphonates in rats.
Although numerous studies have investigated different parameters of laser and ozone therapy, including dose, duration, and application methods, further research is warranted to evaluate the combined use of these therapies in bone healing.