Author(s): Héctor A Corredor*, Carolina Sandoval-Salinas, Jorge Barba, Jose Benitez, Sergio Pusarelli and Andrés F Galleg
There is limited information about the behaviour of erectile dysfunction and premature ejaculation in homosexual and bisexual men. Our objective is to evaluate the clinical and sexual characteristics of the homosexual and bisexual population that consults for sexual dysfunctions in five Ibero-American countries. We reviewed the clinical records of homosexual and bisexual patients over 18 years of age who consulted a specialized institution during 2018. Of 26,650 consultations, 41 patients reported a bisexual sexual orientation (0.15%), and 256 were homosexual (0.96%). The mean age was 42.7 years (+/- 13.5). The mean evolution time for premature ejaculation was 7.6 years, and for erectile dysfunction, it was 5.7 years (+/- 6 months). 46.9% patients reported that these pathologies deteriorated their relationship, and 81.8% reported that they affected self-esteem and confidence. A differential attention should be considered in the sexual health consultation for this population group.
Sexuality, understood as an intrinsic human condition that accompanies individuals throughout their existence and that refers to the individual, social and biological meanings of sex, is a very important factor that distinguishes the gay population from the heterosexual one because the ways in which it operates in its three main functions, reproduction, pleasure and communicating and relating, are particular expressions for this population [1].
In the United States, 4% of the population is gay, and 1% is bisexual; approximately 50 - 79% of gay couples have at least one sexual problem [2, 3]. The approach to sexual dysfunction in the gay population is very variable; understanding, evaluating and treating sexual dysfunctions in this population from a heterosexual perspective have limitations since it is not taken into account that from a biological point of view, the way in which homosexual patients interact sexually is not the same, and the cultural and psychosocial contexts of these relationships are different, requiring a specific focus of attention [1, 3].
Among these differences, homosexual couples take more time in each of the individual sexual practices that generate pleasure and focus less on simultaneous orgasm than heterosexual couples [4]. Similarly, the psychosocial perception of sexual encounters is totally different in homosexual couples since there is no risk of pregnancy. In addition, the positions and roles developed in a sexual relationship can always be interchangeable, something that does not occur in heterosexual relationships [5]. Likewise, noncoital sexuality, such as oral sex, is much more frequent in homosexual couples [6, 7].
Five decades ago, the ten most frequent sexual problems in the no heterosexual male population were described, the most common being their partners’ failure to respond to their sexual needs, while erectile dysfunction and premature ejaculation ranked fifth and eighth, respectively[8]. In a survey of 500 homosexual couples in California, USA, an overall prevalence of erectile disorders of 50% and a prevalence of premature ejaculation of 25% were reported [9]. A study conducted in men who have sex with men found that the prevalence of erectile dysfunction varies according to the age group evaluated, between 15% in men younger than 30 years old and up to 55% in those older than 60 years old. In contrast, the prevalence of premature ejaculation is 17% regardless of age range [10].
The aim of this study is to describe the sociodemographic and clinical characteristics of the gay and bisexual populationdiagnosed with erectile dysfunction or premature ejaculation treated at a sexual health institution in 5 Ibero-American countries during 2018.
A retrospective observational study of the cohort of patients with homosexual or bisexual orientation and diagnosis of erectile dysfunction or premature ejaculation attended at a sexual health institution between January 1 and December 31, 2018, was carried out in Argentina, Colombia, Spain, Mexico and Peru. The data from the medical records were extracted and organized in an Excel® database, which was subsequently exported to Stata15® for the respective analysis of the variables.
Prior to the analysis, the information was validated, and the missing data in the source document and data with extreme or inconsistent values were reviewed. The sociodemographic, clinical and sexual health variables were subsequently evaluated; relative and absolute measures of frequency for the categorical variables and measures of central tendency and dispersion for the numerical variables were estimated globally and by subgroups of interest according to the country and the diagnosis to characterize the research subjects.
297 men reported bisexual or homosexual sexual orientation, out of a total of 26,650 patients attended for erectile dysfunction or premature ejaculation during 2018, in the 5 countries included in the study, which corresponds to 1.11%. Forty-one individuals (13.8%) reported a bisexual and 256 a homosexual sexual orientation (86.2%).
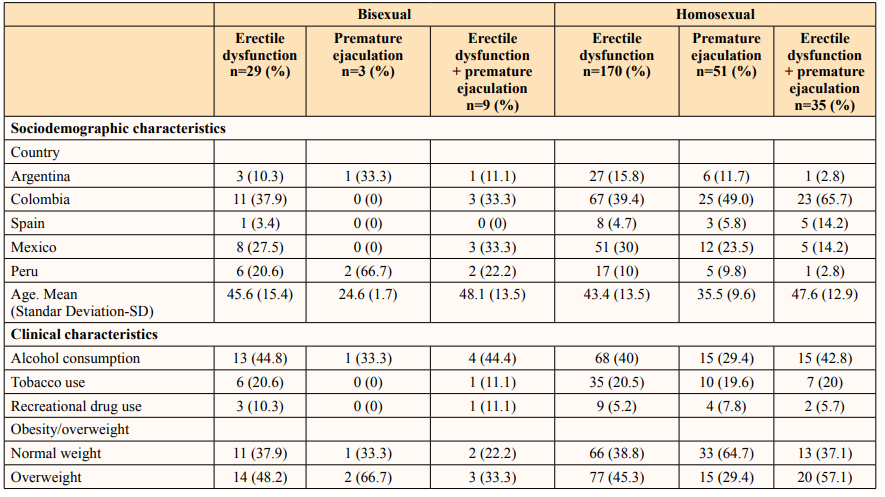
In the general group, the country with the highest number of patients was Colombia, with 129 (43.4%), followed by Mexico (79 patients, 26.5%) and Argentina (39 patients, 13.1%) (Figure 1). The average age was 42.7 years (standard deviation, SD 13.5 years), with a variation between 18 and 82 years. The average body mass index was 22.4 (SD 3.4), 44% of the individuals were overweight, and 11.26% were obese. Of the subjects, 39.1% reported regular consumption of alcoholic beverages (n = 116), 6.4% reported recreational drug use (n = 19), of which the most common was cannabis, and 19.8% used tobacco (n = 59).
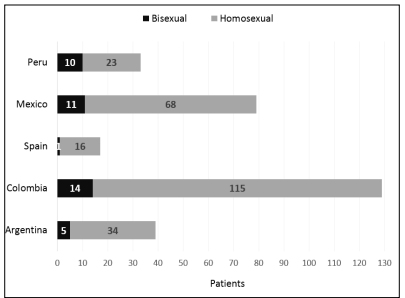
Figure 1: Distribution of homosexual or bisexual patients by country
In the clinical background, 50.8% of the patients did not report any comorbidity (n = 251), 2.6% patients reported genitourinary tract infections (n = 8), 1.3% reported neoplastic pathology (n = 4), 12% metabolic diseases (n = 38) and 13.8% HIV infection (n = 41). Concerning the comorbidities associated with the pathophysiology of erectile dysfunction, 10.7% of patients had diabetes (n = 32), 16.5% had high blood pressure (n = 49), 16.6% had dyslipidaemia (n = 48), 2.0% reported a previous acute myocardial infarction (n = 6), 2.3% had cerebrovascular events (n = 7) and 21.5% reported some psychiatric history (n = 63) (Table 1).
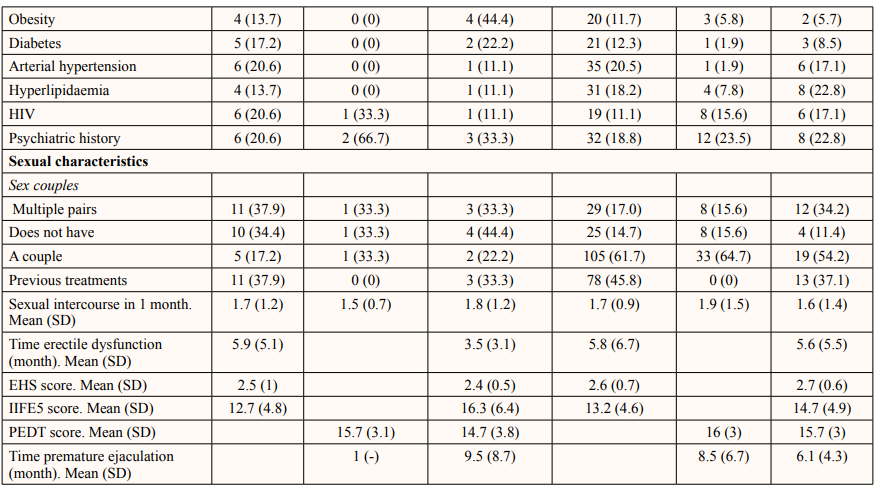
EHS: Erectile Hardness Score; IIEF5: International index of erectile function; PEDT: Premature Ejaculation Diagnostic Tool Relative to the reason for consultation, 199 (67%) patients consulted for erectile dysfunction, 54 (18.8%) subjects consulted for premature ejaculation and 44 (14.8%) suffered from both diseases at the same time (Figure 2). Of the total patient population, 105 (64.5%) had previous treatments for their sexual dysfunctions; 101 patients (41.5%) in the subgroup with erectile dysfunction had been treated with 5-phosphodiesterase inhibitors, and one (0.41%) reported psychosexual therapy.
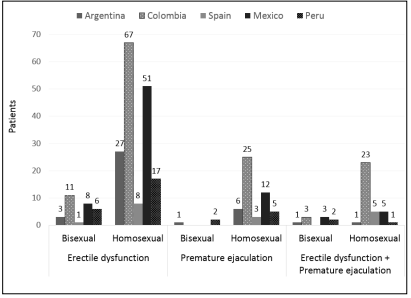
Figure 2: Number of patients according to their sexual orientation by country
In individuals diagnosed with premature ejaculation, 71 cases (72.4%) were lifelong, 25 (25.5%) were secondary, and 2 (2%) presented a syndrome such as premature ejaculation. The median score for the Premature Ejaculation Diagnostic Tool (PEDT) was 16 (range 6-20). Twenty-five patients with secondary disease reported the time of evolution of their disease, which was between 1 and 22 months. Ninety-four subjects (95.9%) reported that their disease generated stress and personal discomfort, and 62 (63.2%) reported that premature ejaculation affected their relationship.
In patients with erectile dysfunction, the median Erectile Hardness Score (EHS) was 3 (range 1-4), and the average of the International Index of Erectile Function-5 (IIFE-5) was 13.4 (SD 4.7). The mean evolution time of the dysfunction was 5.72 months (SD 6.2); 114 (46.9%) patients reported that the pathology deteriorated their relationship with their partner, and 199 (81.8%) felt personally affected by their dysfunction.
Erectile dysfunction and premature ejaculation are two of the most common sexual dysfunctions in the male population [11]. Overall, regarding the epidemiology of erectile dysfunction, a prevalence of approximately 52% is found in people over 40 years of age, while for premature ejaculation, a general prevalence of 31% is estimated according to the survey of social life and national health of the United States [12, 13]. In the gay population, some studies report that approximately 50% of individuals report erectile dysfunction, 19% present premature ejaculation and 44% report having presented premature ejaculation at some point in their life, which would be very similar to the findings in the general population [3, 8, 9]. In our study, we found that 67% of the patients had erectile dysfunction, 18.8% had premature ejaculation, and 14.8% suffered from both diseases.
Regarding the comorbidities associated with these sexual dysfunctions, we found that 31.7% of the individuals in the study had some cardiovascular disease that is related to erectile dysfunction, such as diabetes, dyslipidaemia, hypertension or acute myocardial infarction, which is similar to that reported by other studies, some studies carried out in countries such as Greece and Egypt reported prevalence rates of erectile dysfunction in hypertensive patients ranging between 35 and 43%, the prevalence of syndrome metabolic rate in the population with sexualdysfunction can be as high as 80%, and erectile dysfunction can have a prevalence ranging from 35 to 90% in patients with diabetes mellitus in general population studies[14-18]. To our knowledge, there are no studies about the incidence of these conditions in the homosexual or bisexual population.
An important finding of our study is the history of HIV infection in 13.8% of the research subjects, specifically 12.6% for men with erectile dysfunction and 16.7% in cases of premature ejaculation. According to Luo et al., there is an association between this infection and erectile dysfunction (RR of 2.32; CI 1.52 - 3.55; p-value < 0.001) [17].
Another finding of our study is an unbalanced distribution of patients with nonheterosexual sexual orientation among the countries that were included, observing that 43% of the population is in Colombia and 5% in Spain. These marked differences are possibly due to the lack of reporting in electronic clinical records, which is a weakness of this study due to the retrospective collection of information.
Despite the data reported in this study, it is not possible to assess whether the prevalence of sexual dysfunctions is similar between the heterosexual and nonheterosexual populations because the patients included in our study already had sexual dysfunctions. It will be necessary to carry out studies in the general population to answer this question.
Our results suggest that erectile dysfunction and premature ejaculation behave and are generated in the nonheterosexual population in a different way than in the general population; however, during our research, we found an absence of bibliography regarding the characterization of different sexual dysfunctions in the nonheterosexual population. For this reason, we recommend the development of more studies to obtain more reliable data.
Although this study is descriptive and retrospective, it is of great value since it describes a clearly abandoned population in the sexual sphere. It is important to understand that sexuality as such is not the same in the two populations, and therefore, the perception and experience of these sexual dysfunctions are also not similar; therefore, although statistically they share numbers, averages and medians, the approach, assessment and treatment of these dysfunctions in the gay and bisexual population should be established and planned in a different way than in the heterosexual population. It is here where the work of the sexologist significantly exceeds the medical vision of other professionals, allowing more holistic management of the pathology, with which it is not being concluded that these patients do not require medications, tests or surgery; rather, in addition to such treatments, they should always receive consultation from the sexologist throughout the evaluation and management process.
Other more detailed studies should be carried out in the nonheterosexual population examining the associations between sexual dysfunction and other diseases or comorbidities that could share risk factors, such as cardiovascular pathology, the use of diagnostic questionnaires for sexual dysfunction for these specific populations, adherence to medical treatments, response to behavioural sexual therapy, and even more importantly, evaluating the quality of life impacts of sexual dysfunctions and their treatments in the gay population.
An additional strength of this study is that it evaluates populations from several countries, which makes it easier to extrapolate the results to propose study and treatment behaviours specific to each population [19].
The percentage of homosexual and bisexual men who consult for sexual dysfunctions is low, and their clinical and sociodemographic characteristics are similar to those of the heterosexual population. However, it is important to establish whether differential attention should be considered in the sexual health consultation for this population group that does not currently exist in clinical practice.
We thank each member of the healthcare and logistics teams for our patients in the different countries involved in this research.
Dr. Hector Corredor used information from this research for the presentation of his thesis work for the Masters of Clinical Sexology. The other authors declare no conflicts of interest.