Author(s): Essam Yahiya Al-Shamahi*, Emad Hassan Al-Shamahi, Khaled Abdulkareem A Al-Moyed, Hassan Abdulwahab Al-Shamahy and Azhar Azher Mohammed Al-Ankoshy
Background and Aims: Trachoma has historical and continuing significance as a major cause of vision loss, with an essentially disproportionate impact on the poorest individuals in the poorest communities as in Yemen now under siege and war especially in rural areas. There is no awareness among local and national governments of this disease as a public health problem of top priority in Yemen. However, there is no evidence or no survey/research data or document regarding the prevalence of trachoma in the distract of Bani Matter, in Sana’a Governorate, Yemen. Therefore, we conducted a study to assess the prevalence of active trachoma and associated factors in this rural area.
Methods: A cross-sectional, cross-sectional study was used. A total of 762 children aged 6-12 years participated. We compiled a structured questionnaire from the relevant literature and pre-tested before use. A range of data was collected on social, demographic, and related and environmental factors, facilities and services. The outcome variable was measured using frequencies, cross tabulation, percentage and odds ratio of association.
Results: The gender distribution of study participants was 402 (52.8%) male and 360 (47.2%) female. The study participants were in the age group of 6-9 years (58.9%) while the proportion between 10-12 years was 41.1%. The results of the independent ORs analysis showed that the risk factors for trachoma were: no toilet in the child’s home (odds ratio = 2.3, p = 0.003), orphaned mother (odds ratio = 3.7, p < 0.001), scarce water available in the child’s home (OR = 2.4, p = 0.001), face flies (OR = 2.6, p < 0.001), unclean face (OR = 2.2, p = 0.004), keeping animals in a living house (2.1, p = 0.01), and overcrowding homes (OR = 2.3, P < 0.001).
Conclusion: We define the area in which, at the time of survey among 10–12 children, trachoma was a public health problem in the distract of Bani matter (10.5%) as defined by the World Health Organization (rate ≥ 10%). The implementation of the WHO-approved SAFE strategy for effective prevention and control of trachoma was recommended in the study area due to the prevalence of active trachoma, reaching 10.5% among a group of children above the thresholds recommended by WHO (prevalence >10%). Reducing most of the risk factors in this study depends on health education and provision of the basic things of life to the individual. As for the child losing his parents, especially the loss of the mother, it is a disaster for the child, so addressing causes such as war and poverty for this problem must be a priority in Yemen by the Yemenis themselves, with the help of international organizations such as the United Nations, the World Health Organization and UNICEF
Trachoma, a tropical disease, is the leading infectious cause of blindness in the world. Conjunctival infection is caused by Chlamydia trachomatis. This can lead to the initiation of recurrent episodes of chronic conjunctivitis, which is characterized by the formation of lymphoid follicles. The infection spreads through personal contact (by hands, clothing, or bedding) and by flies that come into contact with secretions from the eyes or nose of an infected person. Trachoma is a disease of poverty that affects more than one billion of the world’s poorest people [1-3]. Trachoma has historical and continuing importance as a major cause of blindness, with an inherently unfair effect on the poorest individuals in the poorest societies. The relatively recent rise in awareness among some national governments about this disease as a high priority public health problem could be due in part to increased financial support from several major donors and the related and highly successful Global Trachoma Mapping Project [4]. The Global Trachoma Mapping Project has been one of the most notable successes of the trachoma community to date, with over 60 partner organizations collaborating at a high speed and in a unified manner. While many countries are facing challenges in disease mapping, global mapping is nearing completion, and as a result, trachoma has been brought to the awareness of health economists [4]. Focusing on Mass drug administration (MDA) antibiotics should not make us forget about the other components of the SAFE strategy. Surgery for individuals with trichiasis is critical. Facial cleanliness, environmental improvement, and associated behavioral changes may be essential factors for eliminating trachoma, but they are not receiving sufficient attention [1-4]. For long-term success, the trachoma community must become improved at selling its progress and latent, as well as by emphasizing the cost-effectiveness of trachoma elimination. There is also a need to ensure that we contribute to the work of the Neglected Tropical Diseases (NTD) community, and undertake deeper engagement with the Water, Sanitation and Hygiene (WASH) sector. These things will help us move closer to achieving trachoma eradication goals, which are now certainly within reach [1-5].
The National Trachoma Program began in Yemen in the 2000s, with funding from the Ministry of Health and Population and international funding. Despite the source of international funding and national guidelines produced, their approaches to implementation were very low. SAFE is not fully implemented in this context. High intake of azithromycin was performed in all cases of endemic trachoma in Hodeidah and Ibb cities according to the NTD and WHO national program, although impact surveys have not yet been conducted [6]. Surgical camps to reduce the accumulation of cases of trichiasis were not ongoing in Yemen. Also, programs dealing with facial hygiene and the components of environmental change in SAFE are absent in Yemen, especially in the time of war, which began in 2015 and continues to this day [6]. Recently Al-Shamahi et al. epidemiological studies were conducted in Bajaj city and Sana’a city, the prevalence of active trachoma among school children was about 10%, and the results of the independent analysis of the accompanying odds ratio showed that the risk factors for trachoma were: Children 7- 9 years, the frequency of washing the face at a rate few per day, flies in the face and/or the child’s unclean face, no parenting education, no water for washing the face and body, no toilet in the house [2,3]. No studies of trachoma have been done in the Bani Matter area before. However, there are a limited number of studies on the prevalence and determinants of eye infection in general and trachoma in particular in Yemen [6-12]. Therefore, the region needs further research to identify the groundwork to reduce the burden of trachoma, especially at the community level that helps government and implementing partners make an evidence- based decision in promoting and providing quality care. The aim of this study was to determine the prevalence and risk factors for trachoma among primary school children living in Bani Matter, Sana’a Governorate, Yemen.
Study Setting: Bani Matter District is located on the western side of Sana’a Governorate, about 30 km from the governorate center (Sana’a city). With a height of 2,674 meters above sea level, it is the most populous area of Sana’a Governorate, with a population of 1,000,012 people. Where Jabal al-Nabi Shuaib is the highest peak in the Arabian Peninsula (3666 m) [13].
This study targeted students of both sexes between the ages of 6 and 12 years, who were selected from public primary schools located in the Bani Matter District, Sana’a Governorate. All children matched the study inclusion criteria a) 6 to 12 years of age, b) study subjects provided informed consent from their parents or other responsible family members and it was provided on the day of examination. Exclusion criteria included: a) non- Yemeni children, b) children medically compromised.
Using EPI version 7, the sample size was calculated, based on the following assumptions: a) The total number of primary students in Bani Matter District is 38078 according to the Ministry of Education. b) The recurrence of previous trachoma is estimated to be around 10%, with a confidence level of 95% and a margin of error of 2.11 [2,3]. From the previous assumptions, it was found that 761 participants (762 were included in the study) were needed to give significant results from the total number of primary school children in Bani Matter.
The multi-stage sampling method recommended by the World Health Organization was chosen, the first stage: from 134 schools, 16 schools were randomly selected: we randomly selected sixteen public schools, representing about 12% of the total number of schools according to the statistics of the Ministry of Education 2018 [14]. For the third stage: in all randomly selected schools, we considered that the study included all categories of students aged 6 to 12 years. Then we randomly choose one category from each level. Finally, the selection was among the systematically randomized categories; To reach the target sample size, which was estimated at 762 children.
A questionnaire was filled out for each child with the child’s personal and clinical data and risk factors. This included age, gender, and clinical information related to eye infections. Also risk factors for conjunctivitis. Experienced examiners, the first author taught general medical students to examine the eye for trachoma and then they performed clinical examinations of the children under their supervision. When a disease case was diagnosed, the cases were photographed and referred to Prof. Dr. Essam Al- Shamahi to confirm the diagnosis. The child’s eye examination was performed according to the WHO classification system for trachoma (Figure 1). The response variable for this study was the presence of a sign of active trachoma (TF/TI) in either of the child’s eyes which could be scored as: The independent variables or risk factors for this study were: sex of the child, age of the child. Frequency of washing the face per day, using soap when washing the face facial hygiene, noting the presence of flies on the child’s face, the child’s parental education level, family size, availability of water in the house, availability of latrines, keeping animals in the living house, the history of the children’s eye discharge, the child’s family members eye discharge, as well as the parental status of the child, i.e.is he/she an orphan, the mother or the father, or both.
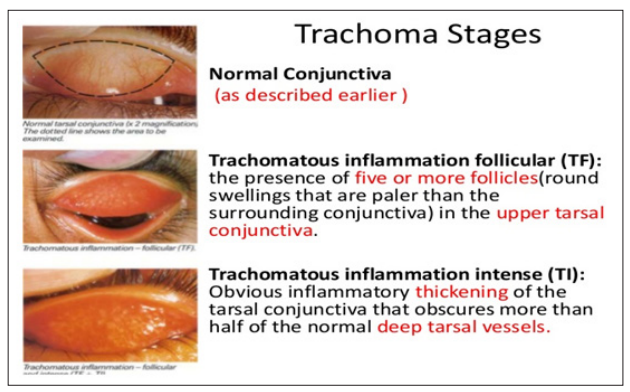
Figure 1: WHO trachoma stages including Normal conjunctiva, TF and TI.
The study was approved by the Research Ethics Committee of the Faculty of Medicine and Health Sciences, Department of Medical Microbiology, Sana’a University.
Clinical, personal, and risk factor data as well as clinical outcomes entered into the questionnaire were analyzed by Epi Info, version7.All children with signs of active trachoma (TF/TI) in either of the child’s eyes were considered to have trachoma. To correlate trachoma positivity and potential risk factors for trachoma, data were examined in the form of case-control studies. For children with trachoma, and unaffected children were matched. Differences in categorical variables were evaluated using Fisher’s exact tests as appropriate. Ninety-five percent confidence intervals (CIs) were calculated for odds ratios (ORs) according to the cornfield limits, and 95% confidence intervals (CIs) were calculated for simple ORs using an exact binomial method. The significance of the difference in ratio and odds ratio was analyzed, and a chi- square (χ2) greater than 3.84 and a p-value less than 0.05 were considered statistically significant.
Table 1 shows the age and sex distribution of children aged 6-12 years who were examined for the prevalence of trachoma in Bani Matter District, Sana’a Governorate, Yemen. Females 47.2% Males 42.8% of the total. The proportion of children in the age group 6-9 years was 58.9%, while children in the age group 10- 12 years constituted 41.1% of the total. The crude prevalence of active trachoma was 9.3% in this study (Table 2), which is slightly similar compared to previous studies by Al-Shamahi et al. In Bajaj, and Sana’a City (10.93%, 9.1% respectively) in 2020 as well as by Thabit et al. 2018 in Al-Dahlia, Al-Hodeidah, Al-Jaws, Hadhramaut, Hajjam, Ibb, Lahj, Marib and Taiz (9%) [2,3-15]. The result of this study showed that children aged 6-9 years had a rate equal to 10.5% and it was slightly higher than the rate of 10-12 years (7.7%) but the difference was not significant (p =0.19) (Table 2). This finding is similar to several other studies, [16-18]. where trachoma is more prevalent at younger ages and the younger age group appears to harbor the greater part of the eye’s C. trachomatis reservoir in environments [17, 18]. A change in trachoma load to higher age groups is observed in areas where the prevalence of trachoma is typically lower, most likely for the reason that transmission intensity (and age of first exposure) is lower in these areas. Despite this, it has been suggested that clinical signs of active ophthalmia trachomatis and C. trachomatis infection separate at lower prevalence [19]. In the current study, 69.3% of children washed their faces less than twice daily as this was a risk factor for trachoma, (OR = 1.9, 95% CI = 1.03-3.4, p = 0.03) (Table 2). The WHO Trachoma Elimination Program encourages face washing as part of the “SAFE” strategy [1,4]. The current study demonstrated a potentially beneficial effect of water and soap-cleaning faces in reducing the odds of developing active trachoma (TI/TF) where washing the face with water and soap at least once per day had an effect on both TF/or TI (2.1 with 95% CI=1.0-4.2, p=0.04) (Table 2). It also showed that other exposures related to hygiene affect active trachoma (TI/TF), such as availability of clean water etc. This result was similar to that reported by Stocks et al. showing a potentially beneficial effect of facial cleaning in decreasing the odds of developing active trachoma (TI/TF) [20]. They included non-randomized studies reporting evidence showing that washing the face at least once per day had an effect on both TF and TI. It also showed that other hygiene-related exposures affect active trachoma (TI/TF), such as: absence of eye secretions, absence of nasal secretions, use of soap, bathing at least once daily and use of towels [21]. These outcomes can be clarified by the significance of the face-washing constituent of the SAFE strategy intended at preserving clean faces in the community with the purpose of decrease eye-seeking flies and person-to-person transmission of C. trachomatis. The promotion of face washing as a community intervention can be joint with mass therapy for people on antibiotics in areas where trachoma is common. Mass treatment with antibiotics aims to decrease the stock of Chlamydia trachomatis in the community, whilst face washing plans to disrupt the cycle of infection and re-infection in the long term [2,3-21]. Emphasize again that children who washed their faces with soap were less likely to have an active trachoma infection. This is due to the fact that using soap in washing the face, the hygiene of the child’s face improves. This reduces the chance of a child developing trachoma and this finding was consistent with previous studies [19,20]. The presence of flies on the children’s face was one more significant risk factor for increasing active trachoma in this study (OR = 2.6, 95% CI = 1.5 – 4.5, p <0.001) (Table 2). Children who did not have flies on their faces were less likely to develop trachoma than children who did not have flies on their faces. This is due to the fact that flies act as a spreading agent of trachoma, transmitting Chlamydia trachomatis from the eyes of infected children to the eyes of uninfected children. This outcome was in harmony with previous studies [2,3-16]. which illustrated that the occurrence of flies on the face increases the opportunity of a child developing trachoma.
|
Age in years |
Gender |
|
|
|
|
|
|
Female |
|
Male |
|
Total |
|
|
|
N |
% |
N |
% |
N |
% |
|
|
6- 9 years |
211 |
58.6 |
238 |
59.2 |
449 |
58.9 |
|
10-12 years |
149 |
41.4 |
164 |
40.8 |
313 |
41.1 |
|
Total |
360 |
47.2 |
402 |
52.8 |
762 |
100 |
|
Variables |
No |
% |
Positive Trachoma N=71 No % |
AOR |
95%CI |
X 2 |
P |
|
Sex |
|||||||
|
Male |
402 |
52.8 |
42(10.4%) |
1.2 |
0.7-2 |
0.7 |
0.37 |
|
Female |
360 |
47.2 |
29 (8.1%) |
1.3 |
0.8-2.2 |
1.5 |
0.2 |
|
Total |
762 |
100 |
71 (9.3%) |
|
|
|
|
|
Age groups |
|||||||
|
6-9 years |
449 |
58.9 |
47 (10.5%) |
1.4 |
0.8-2.3 |
1.7 |
0.19 |
|
10-12 years |
313 |
41.1 |
24 (7.7%) |
0.7 |
0.4-1.1 |
1.7 |
0.19 |
|
Frequency of face washing |
|||||||
|
< 2 |
234 |
30.7 |
14 (6%) |
|
|
|
|
|
≥ 2 |
528 |
69.3 |
57(10.8%) |
1.9 |
1.03-3.4 |
4.4 |
0.03 |
|
Washing face with soap |
|||||||
|
Yes |
169 |
22.1 |
9 (5.3%) |
|
|
|
|
|
No |
593 |
77.82 |
62 (10.5%) |
2.1 |
1.0-4.2 |
4.1 |
0.04 |
|
Face conditions (*No nasal or eye discharge) |
|
|
|
|
|
|
|
|
Clean* |
638 |
83.7 |
51 (8%) |
0.45 |
0.2-0.7 |
8.1 |
0.004 |
|
Unclean |
124 |
16.3 |
20 (16.1%) |
2.2 |
1.3-3.9 |
8.1 |
0.004 |
|
Present of flies on face during investigation |
|||||||
|
Yes |
426 |
55.9 |
52 (12.2%) |
2.6 |
1.5-4.5 |
12.2 |
<0.001 |
|
No |
336 |
44.1 |
19 (5.7%) |
0.4 |
0.2-0.7 |
12.2 |
<0.001 |
|
Education level of Father |
|||||||
|
No education |
147 |
19.3 |
18 (12.2%) |
1.5 |
0.8-2.6 |
1.8 |
0.17 |
|
Primary school above |
615 |
80.7 |
53 (8.6%) |
0.6 |
0.3-1.1 |
1.8 |
0.17 |
|
Education level of mother |
|||||||
|
No education |
488 |
64.1 |
51 (10.5%) |
0.67 |
0.39-1.2 |
2.1 |
0.15 |
|
Primary school above |
274 |
35.9 |
20 (7.3%) |
1.5 |
0.9-2.6 |
2.1 |
0.15 |
|
Availability of water in the living house for face and body wash use |
|||||||
|
Always |
218 |
28.6 |
13 (6%) |
0.53 |
0.2-0.99 |
4.1 |
0.04 |
|
Often |
261 |
34.3 |
18 (6.9%) |
0.6 |
0.35-1.1 |
2.7 |
0.09 |
|
Rarely or absent |
283 |
37.14 |
40 (14.1%) |
2.3 |
1.5-3.9 |
12.3 |
0.0004 |
|
Latrine availability in the house |
|||||||
|
Yes |
656 |
86 |
53 (8.1%) |
0.42 |
0.2-0.7 |
8.5 |
0.003 |
|
No |
106 |
14 |
18 (17%) |
2.3 |
1.3-4.2 |
8.5 |
0.003 |
|
Keeping animals in living house |
|||||||
|
Yes |
513 |
67.4 |
57 (11.1%) |
2.1 |
1.2-3.8 |
5.9 |
0.01 |
|
No |
249 |
32.6 |
14 (5.6%) |
0.48 |
0.3-0.9 |
5.9 |
0.01 |
|
Family size |
|
|
|
|
|
|
|
|
<4 |
126 |
16.5 |
10 (7.9%) |
0.8 |
0.4-1.6 |
0.3 |
0.55 |
|
4-6 |
131 |
17.2 |
14 (10.7%) |
1.2 |
0.6-2.2 |
0.35 |
0.55 |
|
>6 |
505 |
66.3 |
47 (9.3%) |
0.9 |
0.5-1.6 |
0.002 |
0.98 |
|
House overcrowding |
|||||||
|
Yes |
278 |
36.5 |
39 (14%) |
2.3 |
1.4-3.8 |
11.4 |
<0.001 |
|
No |
484 |
63.5 |
32 (6.6%) |
0.43 |
0.3-0.71 |
11.4 |
<0.001 |
|
Has eye glasses |
|||||||
|
Yes |
35 |
4.6 |
4 (11.4%) |
1.3 |
0.4-0.7 |
0.2 |
0.6 |
|
No |
727 |
95.4 |
67 (9.2%) |
0.78 |
0.29-2.2 |
0.19 |
0.6 |
|
History of recent eye discharge |
154 |
20.2 |
21 (13.6%) |
1.8 |
1-2.3 |
4.3 |
0.03 |
|
History of family member eye discharge |
173 |
22.7 |
20 (11.6%) |
1.4 |
0.7-2.3 |
1.3 |
0.39 |
|
Orphan of mother |
71 |
9.3 |
17 (23.9%) |
3.7 |
2-6.8 |
19.8 |
<0.001 |
|
Orphan of father |
169 |
22.2 |
14 (8.3%) |
0.84 |
0.4-1.5 |
0.27 |
0.6 |
|
Orphan of both parents |
31 |
4.1 |
5 (16.1%) |
1.9 |
0.7-5.2 |
1.7 |
0.18 |
*Significant at P<0.05. OR= Odds Ratio, CI=Confidence Interval, p= p value, Χ2= Chi square
In our data, the reported absence of a toilet in the child’s home (open defecation) was associated with higher odds of active trachoma in children (OR = 2.3, 95% CI = 1.3–4.2, p = 0.003) (Table 2), as also seen previously [2,3-9]. This is consideration to be related to the fact that Musca sp. flies lay their eggs on exposed surface human faces [2,3]. It has been recommended that the provision of enhanced latrines could reduce the fertility of these flies and thus reduce transmission of ocular C. trachomatis in areas where flies are a significant vector [2,3]. On the other hand, the degree to which latrine use directly affects the strength of infection is unclear, in as much as latrine use can also represent a proxy for other parameters that affect health, such as education or economic opportunity. This disease continues in a lot of parts of the developing world, in communities that lack access to adequate water and sanitation [2-4]. This study discovered that children with home water rarely or absenteeism were 2.3 times (OR = 2.3, 95% CI = 1.5 – 3.9, P= 0.0004) more likely to have active trachoma compared with home children with constant availability of water in their complex. This may be due to the importance of water for facial and personal hygiene. Facial hygiene is one component of the SAFE strategy. To implement this strategy, the availability of water is critical to reduce the transmission of trachoma. This result was consistent with other studies [2-23].
Different groups use diverse definitions to name orphans. One of the legal meanings used in the United States is a minor disenfranchised through “death, disappearance, desertion or desertion of both parents, separation or loss of both parents” [24]. In common usage, an orphan has no surviving father to look after him. However, the United Nations Children’s Fund (UNICEF), the Joint United Nations Program on HIV and AIDS (UNAIDS), and other groups describe any child who has lost a parent as an orphan. In this method, a mother orphan is a child whose mother has died, a paternal orphan is a child whose father has died, and a double orphan is a child/adolescent/infant who has lost both parents. This contrasts with the older use of orphans to describe children who have lost only one of their parents. Orphans are fairly rare in developed countries, for the reason that most children can expect their parents to stay alive their childhood. There are much larger numbers of orphans in war- torn countries such as Yemen. Wars, epidemics (such as AIDS), and poverty have resulted in many children becoming orphans.
In Yemen the significant causes of orphans are war and poverty [25,26]. The catastrophic consequences of war in Yemen, which include the loss of a female parent, a male parent, or both. This study revealed that children of a missing mother were 3.7 times (OR = 3.7, 95% CI = 2 – 6.8, p < 0.001) (Table 2) more likely to have active trachoma compared with children with a father (mother). This might be due to the importance of mother in caring children on matter of hygiene, nutrition’s and psychological care. One of the components of SAFE strategy against trachoma must be applied policy to help and care for those fragile group of the society. To implement this strategy, availability of health care and nutritional personal in primary schools in Yemen are crucial to reduce the transmission of trachoma. This association was not mentioned before in other studies in African and Asian countries [2,3,16-21]. Socities must follow many religious texts, including the Bible and the Qur’an, which contain the idea that helping and defending orphans is very important and pleasing to God. The two religious’ leaders, Moses and Muhammad, were orphaned as children. Numerous citations in the Qur’an and Bible describe how orphans are treated and cared for.
In Yemen, the monitoring and evaluation process takes place centrally. Although the management approach is based on the SAFE strategy, it differs from the standard WHO recommendations that should target the community level in Yemen. The main focus should be on children of school age. In communities where trachomatous inflammation—follicular (TF) in children aged 6-9 years is ≥10%, antibiotic therapy is given every 6 months. Programs should also be developed to promote facial hygiene. In addition to having a strong link to primary care is critical, including surveillance as part of routine methods as our previous and current studies performed [2,3].
The authors would like to acknowledge Sana’a University, Sana’a, Yemen and The Eye Consultation Center, Sana’a city, Yemen for their supports.
“No conflict of interest associated with this work”.
All authors participated on this survey by trained the survey tem and supervising the clinical works and the reviewing and editing the research document.