Author(s): <p>Ali Alsmair</p>
A 54-year-old man with type 2 diabetes mellitus presented with limitation of movement, flexion deformity and stiff skin of both hands. The diagnosis was suspected clinically. Both wrists MRI were requested, however only the right wrist MRI was obtained for financial conditions
Diabetic cheiroarthropathy, also named Diabetic stiff hand syndrome, Pseudoscleromatous hand of the diabetic and diabetic sclerosis, is characterised by painless movement limitation of the hands' small joints. It is mainly a clinical diagnosis and is known to have an association with microvascular ischaemic disease [1].
Diabetic cheiroarthropathy can be seen in 30% of poorly controlled patients. The patient's usually cannot fully extend the fingers, due to the accumulation of sugar alcohols around the flexor tendons [2].
A 54-year-old diabetic patient presented with mild hand swelling, limited motion of both hands, flexion deformity, and inability to extend his fingers. No erythema. Negative Tinel's test. No signs of Dupuytren's contracture. No dysphagia. No eye or mouth dryness.
Firstly, the patient was suspected to have rheumatoid arthritis, however, there was no good response to anti-inflammatory drugs and inflammatory markers were normal. HbA1c was requested and was 8.7%. The patient was positive for both the "Prayer sign" and "Tabletop sign". The clinical findings along with elevated HbA1c were highly suspicious for diabetic cheiroarthropathy, so MRI was obtained for confirmation and mainly to exclude other possibilities.
MR images showed thickening and oedema of the flexor digitorum tendons and flexion deformity of the hand.
The main DM musculoskeletal findings include Diabetic cheiroarthropathy, Dupuytren's contracture, carpal tunnel syndrome and myonecrosis [3].
Diabetic cheiroarthropathy can be seen in both DM1 and DM2. It is mainly a clinical diagnosis. The main clinical signs are limitation of movement of the hands' small joints, stiff skin of the dorsal aspect of the hand and positive "Prayer sign" and "Tabletop sign"[1].
The Prayer sign is defined as the inability to approximate the palmar surfaces of the palms and interphalangeal joints of both hands to each other in the prayer position [3].
The tabletop sign is an incomplete contact of the palmar surface of the fingers of the hands with the tabletop when the patient is asked to put the hands’ palms down on the tabletop [3].
The pathogenesis of diabetic cheiroarthropathy is multifactorial, including glycosylation of the collagen, which proliferated in the skin and tendons, and diabetic microangiopathy of the skin and subcutaneous vessels, resulting in skin stiffness [1].
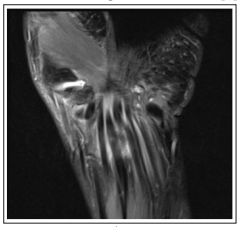
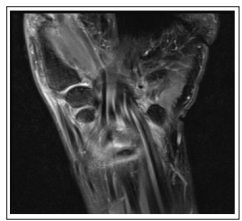

Figures: A, B and C, Coronal T2 fat-sat images of right wrist/ hand show oedema and thickening of the synovial sheaths of all the flexor tendons at the wrist and hand level.
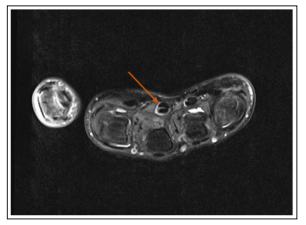
Figure D: Axial T2 fat-sat image, shows thick oedematous synovial sheath of the flexor digitorum and superficialis tendons.
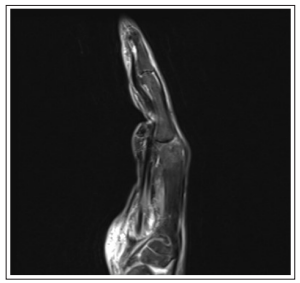
Figure E: Sagittal T2 fat-sat image shows flexion deformity of the hand.
Diabetic cheiroarthropathy is mainly a clinical diagnosis and can be reversible if early treated. It can be considered as an alarm for other associated microvascular complications of diabetes mellitus. MRI is useful to exclude other musculoskeletal manifestations of diabetes and other causes of flexor digitorum tendons synovial thickening [3].
1. Cherqaoui R, McKenzie S, Nunlee-Bland G (2013) Diabetic Cheiroarthropathy: A Case Report and Review of the Literature. Case Reports in Endocrinology 2013: 1-3.
2. West S (2012) Systemic Diseases in Which Arthritis is a Feature. Goldman's Cecil Medicine 2: 1747-1752.
3. Khanna G, Ferguson P (2007) MRI of Diabetic Cheiroarthropathy. AJR Am J Roentgenol 188: 94-95.
View PDF