Author(s): Dereje Feleke, Gosaye Tekelehaymanot Zewde*, Astawus Alemayehu, Asefa Tufa, Abdusemed Abdurahman, Abebaw Demissie, Mohammed Yusuf and Zelalem Bekele
Background: COVID-19 is not well studied in Ethiopia, especially in the eastern parts of the country. Determining the clinical profile and treatment outcome of COVID-19 cases will help to plan better prevention and treatment strategies considering the local context. So, this study attempted to investigate and describe the Clinical characteristics and outcomes among hospitalized COVID-19 patients.
Methodology: Institutional based retrospective study design was used. The data extraction tool was prepared by using the COVID-19 log-book template and data was collected from 2091 COVID-19 confirmed patients using RT-PCR (real-time polymerase chain reaction) testing method who were admitted at three COVID-19 treatment centers from 21-May-2020 to 02-Aug-2021. Data was entered in Epi-data version 3.2 and analysis was done by SPSS version 25.0. Descriptive statistics proportions, percentages, ratios, frequency distributions, measures of central tendency, and dispersion were used. The result was presented in thefigure and table.
Result: A total of 2019 patients were analyzed. In this study majority, 1309 (62.6%) of patients were male and the age ranges of patients were from 8 months up to 100 years with a mean age of 33 years and the most predominant age groups were less than 30 years. Around a quarter of 478 (22.9%) patients were symptomatic and the three most common symptoms manifested were cough 437 (20.9%), shortness of breath 210 (10%), and generalized body weakness 206 (9.9%). The prevalence of comorbidity was 105 (5%), of which DM 37 (1.8%), Hypertension 22 (1.1%) and CVD 15 (0.7%) were the most common. In this study 1992 (95.3%) of COVID-19 patients were recovered and 77 (3.7%) died.
Conclusion: This institutional-based COVID-19 register review showed that the most common clinical manifestation were cough, shortness of breath, and generalized body weakness and among the admitted patients male accounts for the lion shares of the number. Majority of patients were asymptomatic this will increase asymptomatic transmission in the community, thus effort community mass screening intervention is important.
Coronavirus (COVID-19) is an emerging infectious disease caused by a newly discovered coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-COV-2) and it has emerged as a human-infecting beta-coronavirus which had previously not been detected in humans or animals. It is named COVID-19 by the World Health Organization (WHO) and SARS-CoV-2 by the International Committee on Taxonomy of Viruses as it is similar to the coronavirus responsible for the severe acute respiratory syndrome (SARS-CoV) [1,2].
The WHO declared the COVID-19 outbreak as the sixth public health emergency of international concern and also declared the outbreak as a pandemic and it is transmitted from person to person via respiratory droplets, contact, and aerosols. It is characterized as highly fatality in severe cases, and with no specific medicine, it poses a huge threat to human life and health. [3,4].
COVID-19 is currently spread to almost all countries of the world at the start of the outbreak, the global pandemic has surpassed 97.8 million cases worldwide with more than two million deaths by January 21, 2021 [5].
The disease had well notified clinical manifestations which will appear in as few as two days, or as long as 14 days after exposure [6]. However, there is concrete evidence to suggest that human-tohuman transmission may be occurring during the asymptomatic incubation period [7].
The first instance of COVID-19 in Sub-Saharan was reported on 28 January 2020 in Nigeria and has now speared to all of Sub-Saharan Africa [8]. In Ethiopia the first COVID-19 case was identified on March 13, 2020, since then, the number of new cases in the country has been rapidly increasing. As of March 10, 2021, the country had 168,335 COVID-19 positive cases and 2451 deaths domestically [9].
Some scientific research has been done on many features of COVID-19, but still localized valid, and reliable information is needed to intervene properly. In the same manner, so far there are no concrete and systematically designed studies about the magnitude and characteristics of this disease at the regional and country-level except the report of daily time series of confirmed cases, recovered cases, and deaths, with a representative sample size. Furthermore, in Ethiopia primarily due to insufficient health facilities, few testing sites, low testing capacity, delayed case reports, and poor recording and documenting practice the total number of cases might be underestimated and expected to be more than what is being reported. As a result, the exact current figure needs to be known, and the distribution among various regions of the country needs to be identified. So, this study attempted to determine the Clinical features & treatment outcomes of COVID-19 patients in treatment centers in Eastern Ethiopia.
The study was conducted at Harar town which is found in the eastern part of Ethiopia 525 km away from the capital city of Ethiopia and the estimated total population of the region is 246,000 [10]. The study was conducted in Hiwot Fana Specialized comprehensive University Hospital, Jugal Hospital, General Hospital, and Turkey treatment center from February 28 up to March 18, 2022.A retrospective cross-sectional study design was used
Study Populations and Eligibility Criteria: The study participant was all patient records that were tested positive for COVID 19 using the golden testing techniques, RT-PCR method, and who had contain a complete and accurate record.
Sample Size Determination: All 2091 COVID-19 patients admitted to treatment centers from 21-May-2020 to 02-Aug-2021 and fulfilled inclusion criteria were included.
Data Collection Tools and Procedure: Data was collected from the registration logbook, COVID-19 intake forms. The data extraction tool consists of socio-demographic, Presence and types of co-morbidity, Clinical characteristics during admission, severity status, and treatment outcome of patients. Six trained health professionals who have been working in the treatment center collected the data.
Data Quality Assurance: Data quality assurance mechanisms were instituted at several points to ensure the quality of the data. A pre-test was done on 5 % of the total sample and training was given to thedata collector and supervisor for two days. All the extracted data was checked for accuracy and completeness on daily basis. The data was coded carefully to increase the level of accuracy. Data Process and Analysis: After data were collected, entered into Epi-data version 3.2 and then exported to SPSS version 25.0 for analysis. It was cleaned and edited (checking for missing values and outliers). The Univariate analysis such as proportions, percentages, ratios, frequency distributions, measures of central tendency, and measures of dispersion was calculated. The result was presented by the graph, table as well as narration
Ethical Considerations: Ethical clearance letter was obtained from Harar Health Science College Research Ethics Review Committee and it was submitted to the study organization consent was obtained from the hospital CEO and Permission was obtained from the study institution.
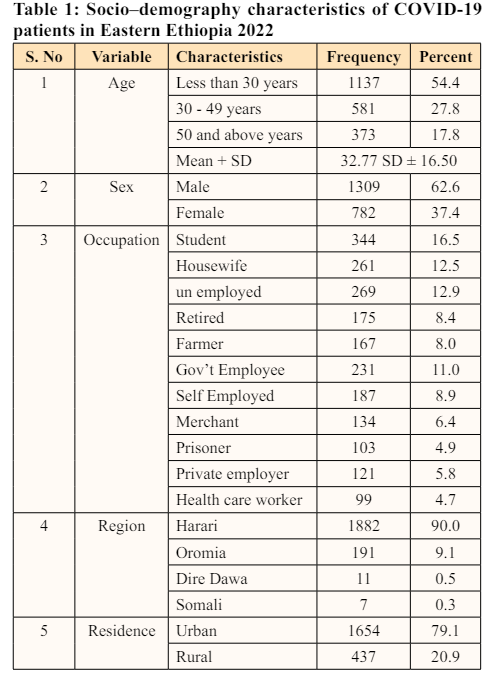
A total of 2091 patients recorded with COVID 19 were enrolled in this study. The majority 1137 (54.4%) of patients were less than 30 years old, with a mean age of 32.77 and a standard deviation of (SD ± 16.50). Most of the patients 1396 (62.6%) were male. Among the participants, 344 (16.5%) patients were students by occupation, and 1882 (90.0%) patients were from the Harari region. One third 1654 (79.1%) of the participants were urban dwellers (Table 1)
Among 2091 patients approximately a quarter of 478 (22.9%) were symptomatic while the rest 1613 (77.1%) were asymptomatic. The three most common prevalent clinical features among symptomatic cases were cough 437 (91.4%) shortness of breath 210 (43.9%) and generalized body weakness 206 (43%) (Figure1).
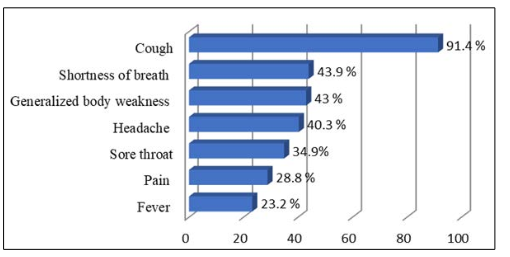
Figure 1: Type of symptoms among COVID 19 patients in Eastern Ethiopia 2022
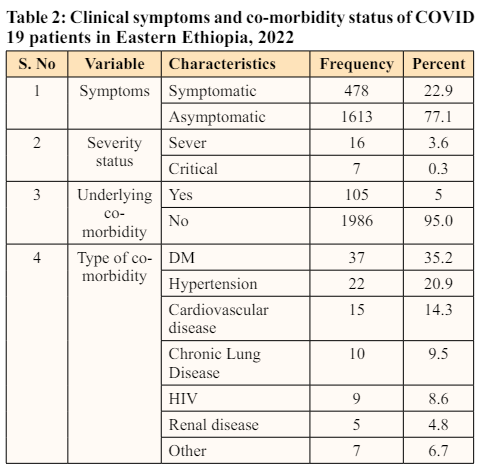
Among the total 2091 COVID-19 patients, approximately a quarter of 478 (22.9) patients were symptomatic, of which 1948 (93.2%) were mild, 60 (2.9%) moderate, and 16 (3.6%) were severe, whereas 7 (0.3%) were critical symptoms at the time of admission. Only 105 (5%) of patients had medical co-morbidity, of which DM 37 (35.2%), Hypertension 22 (20.9%), CVD 15 (14.3%), and Chronic Lung Disease 10 (9.5%) were the most common (Table2).
Among 2091 COVID 19 patients were admitted to the treatment center 1992 (95.3%) patients were recovered and discharged while 77 (3.7) patients died and 16 (0.8%) transferred out and 6 (0.3%) were lost from the treatment center (Figure 2)
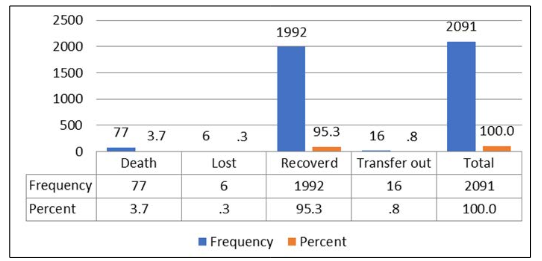
Figure 2: Clinical outcome of COVID 19 patients in Eastern Ethiopia 2022
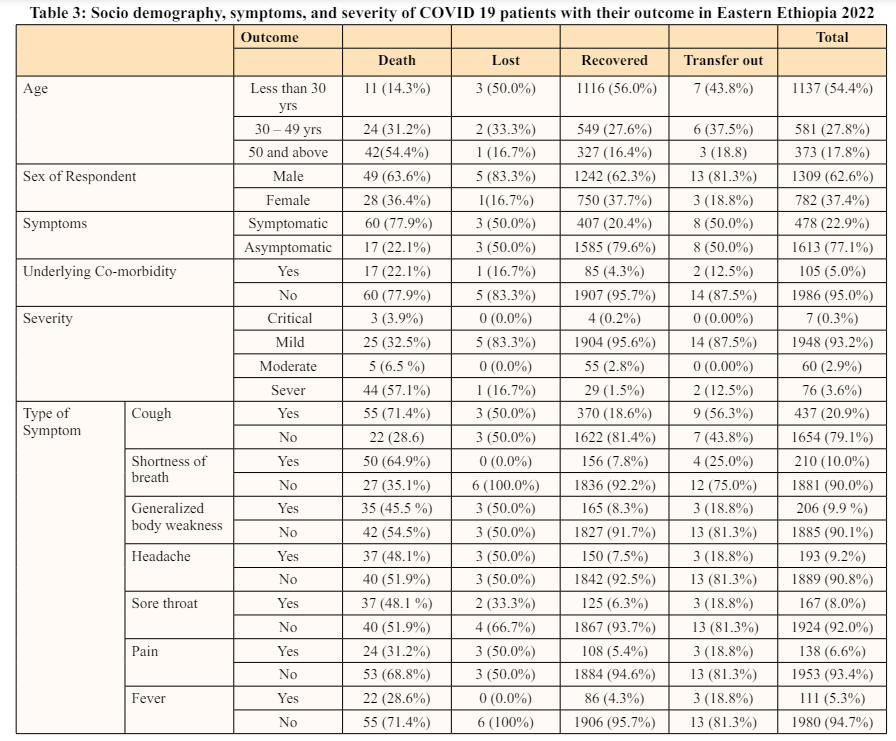
Even if more than half 1137 (54.4%) of patients were found in the age group less than 30 years few 11 (14.3%) patients have died. Among 77 dead patients majority of 42 (54.4%) were above 50 years. In comparison to male and female sex death rates 49 (63.6%) as well as COVID-19 acquisitions, 1309 (62.6%) were highest among males. In those patients who do not have underlying Co-morbidity, 60 (77.9%) was high death rate than 17 (22.1%) for those with having comorbidity. In this study most 1613 (77.1%) patients were asymptomatic, in contrast, the frequency of death was higher in symptomatic 60 (77.9%) than asymptomatic once. Frequently a large number of 25 (32.5%) death observed in mild cases. The most common symptoms with the frequent number of patient death observed were Cough 55 (71.4%) followed by shortness of breath 50 (64.9%) (Table 3).
This study included all the 2091 COVID-19 cases that were admitted to Hiwot Fana specialized University Hospital, Jugal General Hospital, and Turkey COVID-19 treatment centers. In this study, we found that most confirmed COVID-19 cases were in an age group of fewer than 30 years. The majority of patients admitted with COVID-19, who recovered, and died were males. Most asymptomatic patients had a higher frequency of recovery. Co-morbidity is one of the underline factors for disease worsening in the case of COVID-19. In contrast to this fact, in this study, the majority of patients without underlined co-morbidity died more than those having co-morbidity.
In this study majority of patients were male (62.6%) this finding was in line within most literatures elsewhere in Pakistan (70.25 %) [11] Wuhan from China (53.8%) [12] Northern Ethiopia (63.3%) [17], (south Ethiopia (55.9%) [20] (Addis Ababa (71%) [26] Ethiopia treatment center (69.5%) [23]. This finding suggested that the prevalence of COVID-19 infections was highest among males. In this study finding, the majority of patients were aged less than 30 yrs, which is not in line with studies conducted in [11,22,24] majority of patients aged were above 50 years. This difference might be due to the sample size.
Our findings showed that among recovered patients (16.4%) were beyond the age group of 50 years, while (27.6%) were between 30-49, whereas (56.0%) were <30 years, and (62.3%) were male. This finding is lower for the age group of 50 years (48.5%), and between 30-49 years (27.6%), but higher for less than 30 years (56.0%) and male sex (62.3%) when compared with the study conducted in Dill University [20]. This may be due to difference in sample size and socio-demography.
Regarding death and sex in our study, 62.6% of dead patients were male, this is higher than the study conducted in Brazil [15] (55.4%) Dilla University [20] (57.1%), but also lower than (71%) study conducted in Ethiopia [26].
In our study, 77.1 % of the patients were asymptomatic; the finding was higher as compared to the studies conducted in North Ethiopia (50.6%) [17], In Ethiopia (73.8%) [18], and Addis Ababa (20.8%) [26], this may be the alarming point, which indicated that a large number of community members were at risk of getting infected with these asymptomatic cases. In contrast to the above findings, the prevalence of asymptomatic cases was higher in (85%) of North-East Ethiopia [22]. This discrepancy might be due to the sampling size and study period.
COVID -19 patients may have different clinical features, in our study the most prevalent clinical manifestation were cough (91.4%) shortness of breath (43.9%), and generalized body weakness (43%) the finding is lower than study conducted in Boru- Meda Hospital cough (67.1%) and shortness of breath (31.5%) [23]. On the contrary, it was higher than study conducted in China Cough 13 (100%) and Fatigue 8 (61.54%) [12] and Dilla University Referral Hospital Treatment Center cough (95%), shortness of breath (69.5%) [20] This variation may be due to sample size, study population and living area.
Our findings illustrate that the most common co-morbidity of the COVID-19 patients were DM (35.2%), Hypertension (20.9%), CVD (14.3%) Chronic Lung Disease (9.5%), and HIV (8.6%) our finding was higher than other studies done in Dilla University hypertensive [20] (20.9%) type II Diabetes Mellitus, (14.5%), North Wollo [22] Diabetes mellitus (1.1%), Hypertension (1.6), HIV (1.6%), and chronic respiratory diseases (1.1%) and (South Central, Ethiopia)(24) Diabetic Mellitus (28.0%), Hypertension (16.1%) Chronic cardiac disease (10.6%) Chronic kidney disease (4.3 %) but also lower than study conducted in Addis Ababa (26) DM, (48.9%) Hypertension (27%), HIV(17.6%) were the most common co-morbidity. This difference might be due to the age of the participant, sample size, and socio-demographic conditions.
In our study, most deaths happened in males (62.6%) than in female sex; this finding was in line with a study conducted in Brazil [15], Dilla University Referral Hospital Treatment Center [20], and Addis Ababa [26].
In this study, 77 (3.3%) of COVID-19 patients had died; this finding was in line with a study conducted in North Ethiopia. [0.8%] [21] while lower than studies from China (28.27%) [13], Wuhan pulmonary Hospital (11.73%) [14], Belgium (29.9%) [16] Ethiopian findings (1.9%) [19], Dilla University Referral Hospital Treatment Center (22.3%) [20], and Wollega University Referral Hospital (5.7%) [25]. This finding showed that there was a lower death rate in our study than in others; it may be due to differences in quality of care, presence of sufficient treatment centers in relation to geographic area, sample size, and socio-demography
To the best of the authors’ knowledge, this study is one of the first comprehensive assessments of the clinical condition and treatment outcome of COVID-19 patients admitted to COVID 19 Treatment center in eastern Ethiopia. The study also provided the most relevant information on comorbidity, severity status, and death related to COVID-19. In this study, we found that most confirmed COVID-19 cases were aged less than 30 years, particularly males. Among patients with a sign and symptoms cough, shortness of breath, and generalized body weakness was the most common clinical manifestations while Chronic Lung Disease, HIV, and renal disease were less frequent.
The majority of SARS-CoV-2 infected patients were symptomatically making the community more at risk of being infected and increasing asymptomatic transmission in the community. DM and HPN were the two most common comorbidity. The majority of COVID-19 patients recovered followed by death. As per the findings from the current study, we can conclude that there is most patient death occurs in the age group of fewer than 30 years and in those asymptomatic patients. Patients who had seriously ill were a high chance of death. Therefore effort needs on community screening for role outing contact tracing of asymptomatic cases as well as improvement of health care seeking behavior of people.
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
The authors declare that they have no conflicts of interest.
This work received no public or private funds.
Any time, the corresponding author provide an additional resource request