Author(s): Fahim Aslam
Dengue virus is one of major public heath burden in several countries, it is described to be “a fast-emerging pandemic prone viral disease” by the WHO and is one of the most common form of vector borne diseases worldwide. The disease is transmitted through the female Aedes mosquito and most commonly found in tropical countries. A reported 400 million reported dengue cases occur yearly and an estimated 3 billion people could be affected by the disease in the upcoming decade making it a global crisis. The disease is caused by four serotypes of the dengue virus (DENV1-4) making it difficult for the treatment to work on the patients due to its different virulent mechanism. Using the data available from the Ministry of Health, Epidemiology Unit in Sri Lanka the dengue reported cases from 2014 to 2018 are analyzed over the five years to identify the trends and occurrence patterns [1,2].
Dengue virus was initially discovered in the Chin Dynasty (265- 420AD) and known to be a mosquito borne viral infection. The disease has four serotypes in common, DENV1, DENV2, DENV3 and DENV4 which arises from the same family of genus flavivirus. The aedes aegypti mosquito is known to be the primary vector for dengue and the disease can be transmitted through a female mosquito bite [3,4]. Patients infected with dengue virus shows signs of high fever (40°C or more) and common signs of headache, nausea, muscle and joint pain, swelling of the lymph nodes and rash in general. High fever accompanied with any of the two above symptoms indicates the patient is suffering from dengue according to the WHO guidelines. Dengue was classified into two main categories in 2009 where, dengue ± warning signs and severe dengue being the two criteria designed to suit the epidemiology of dengue [1].
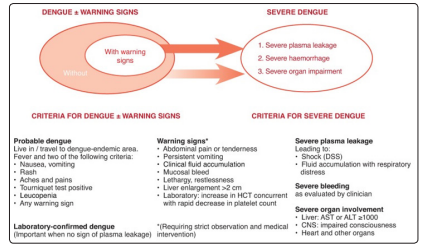
Figure 1: 2009 Classification of Dengue [5]
A reported 400 million people are affected by dengue every year and 25% of the reported cases have the severe dengue manifesting in the body. Asian countries contribute to nearly 50% of the cases of dengue mainly among the subtropical countries such as Thailand, Indonesia, Philippines, India, Bangladesh and Sri Lanka most commonly. The disease is most common during rainy seasons of the year as the dengue mosquitoes are able to survive, breed and increase larvae formation at sites of water collection. As dengue contains four serotypes it makes it difficult to prevent the action of dengue mosquitoes and since the mosquitoes contain a short reproduction cycle, the number of eggs laid during the rainy season can cause an increase in mosquitoes leading to high number of reported cases [6,7].
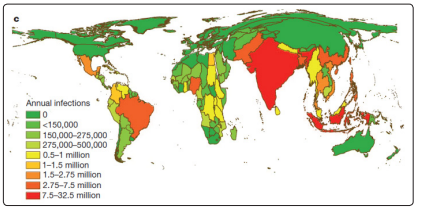
Figure 2: Global Incidence of Dengue Fever Shows Asia Having the Highest Proportion of Dengue Occurrences [6].
Sri Lanka is an island country situated closer to the equator and contains two main weather patterns, the wet and dry seasons. The most common being the first inter monsoon season which occurs during the months of March and April and the second inter monsoon season which occurs during October-November. Due to the unpredictable weather changes and humidity being ideal for mosquitoes to breed in, the number of reported dengue cases have been fluctuating over the past five years. This has led to Sri Lanka being endemic to dengue disease as the climatic conditions are suiting the overall dengue breed and growth. According to a study carried out by, the most common serotypes affecting Sri Lanka are DENV2 and DENV3 being the most prevalent from1900?s. Most recently the DENV 1 outbreak was observed in Colombo in 2009 where a sudden surge in the number of dengue patients increased [8,9].
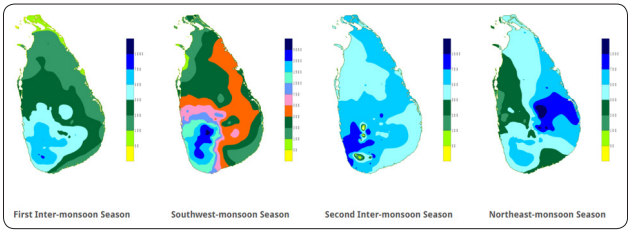
Figure 3: Monsoon seasons in Sri Lanka [11].
The data for reported dengue cases was obtained using the Ministry of Health, Epidemiology Unit of Sri Lanka from 2014 October to 2019 October. Using the data available descriptive statistical analysis was carried out to observe changes and trends in the available data. Pearson R correlation was carried out to identify relationships between the monthly data points. Time series forecasting was carried out to estimate the data for 2019 using the available dataset.
| Month | 2014 | 2015 | 2016 | 2017 | 2018 |
| January | 3610 | 6345 | 6694 | 10927 | 7278 |
| February | 2011 | 3731 | 4439 | 8724 | 4490 |
| March | 1648 | 1962 | 2696 | 13540 | 3380 |
| April | 1682 | 1293 | 2832 | 12510 | 2618 |
| May | 4292 | 1625 | 2422 | 15936 | 3560 |
| June | 6736 | 1477 | 4731 | 25319 | 5513 |
| July | 5721 | 2125 | 10715 | 41121 | 6455 |
| August | 4022 | 1604 | 4873 | 22270 | 4293 |
| September | September | September | 3629 | 9519 | 2049 |
| October | 4297 | 2066 | 2185 | 6614 | 1905 |
| November | 5452 | 2762 | 2257 | 8868 | 4537 |
| December | 5391 | 3688 | 7677 | 10753 | 5581 |
| Total | 47502 | 29777 | 55150 | 186101 | 51659 |
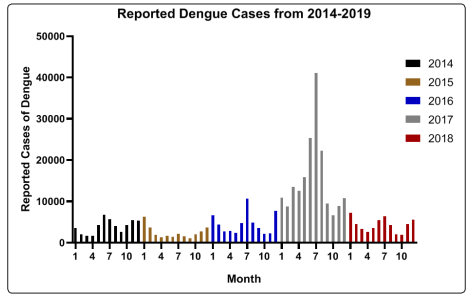
Figure 4: Comparison between Months of Reported Dengue Cases From 2014-2018
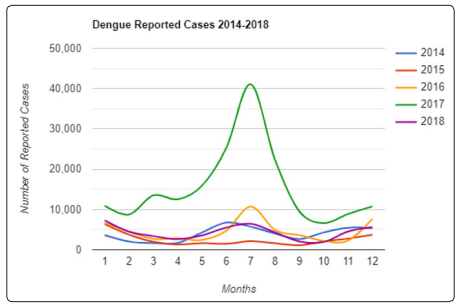
Figure 5: Trendline Graph of Dengue Reported Cases
| 2014 | 2015 | 2016 | 2017 | 2018 | |
|---|---|---|---|---|---|
| 2014 | 0.007058 | 0.407223 | 0.477781 | 0.500025 | |
| 2015 | 0.007058 | 0.366371 | -0.26415 | 0.66767 | |
| 2016 | 0.407223 | 0.366371 | 0.664855 | 0.762473 | |
| 2017 | 0.477781 | -0.26415 | 0.664855 | 0.467654 | |
| 2018 | 0.500025 | 0.66767 | 0.762473 | 0.467654 |
| Descriptive Measures | 2014 | 2015 | 2016 | 2017 | 2018 |
|---|---|---|---|---|---|
| Minimum | 1648 | 1099 | 2185 | 6614 | 1905 |
| Maximum | 6736 | 6345 | 10715 | 41121 | 7278 |
| Range | 5088 | 5246 | 8530 | 34507 | 5373 |
| Mean | 3959 | 2481 | 4596 | 15508 | 4305 |
| Std. Deviation | 1692 | 1490 | 2613 | 9815 | 1699 |
| Std. Error of Mean | 488.6 | 430.2 | 754.4 | 2833 | 490.4 |
| Skewness | -0.013 | 1.797 | 1.328 | 1.880 | 0.195 |
| Kurtosis | -1.130 | 3.485 | 1.444 | 3.681 | -0.769 |
Dengue in Sri Lanka is a growing concern with increasing trends of the disease presented over the past decade. As shown above in table 1, a high number of reported cases have been observed over the past five years with the highest reported cases observed in 2017 where 186101 patient cases were recorded. This was mainly due to the continuous monsoon season where heavy rainfalls were reported throughout the country with flash floods. In contrast, the rainfall levels were comparatively less with increased temperature in 2015 which could have led to reduced mosquito breeding and reproduction [18]. An overall increase of the reported dengue cases is seen over the course of five years, where the Pearson R correlation values were calculated to identify the change in mean differences. An overall R value of 0.50 was observed during the course of 2014-2018 showing an increasing positive trend in repeated number of cases. In table 3, the descriptive statistics measures show an overall skewness lies within -1.96 to 1.96 indicating that the data available is normally distributed. Figure 3 justifies this statement where the data shows a right tailed bell shape curve as a peak is observed in 2017 due to the increased incidence of dengue reported cases. Figure 4 shows the similar trendline patterns observed over the five years where the common peak being observed at the 4th, 6th and 9th months of the year where the monsoon season is prevalent.
This disease affects the economy of the country where around one hundred thousand LKR is spent on an individual during dengue fever stages. The greater number of patients affected annually increases the healthcare cost and maintenance of patients in hospitals [13]. In addition to the available four types of dengue serotypes a new serotype, DENV-5 has been found in 2013 showing signs of the dengue virus developing resistant strains which can lead to more deaths globally [16].
Early diagnosis and creating awareness have been identified as the main goal in eradicating the disease, WHO has encouraged the use of awareness programs to prevent excessive breeding of mosquitoes [12]. Due to the limitations presented in low-middle income class country the most common method of testing used for dengue diagnosis is PCR, although the method is accurate it takes time for the result to be given and is considered to be one of the outdated techniques in modern world. NAAT and NSI-based assays are used in South American and North American countries as an early and more reliable method of testing [17].
Treatment options for dengue are limited in only curing the symptoms as there is no anti-viral therapy as of now due to different serotypes presented. Recent findings have been able to identify dengue vaccines to cure children and young adolescents but as of now there has several complications regarding the use of the vaccine in endemic regions [15]. As stated by [14] due to the lack of knowledge and vector surveillance programs, the endemic of dengue infections will only begin to rise in low income countries which can lead to increase in morbidity and mortality. In Sri Lanka despite awareness programs being conducted on a regular basis, there is lack of implementation among the general public and environmental maintenance workers. Due to this, mosquitoes are able to breed in sewages and garbage disposal sites which causes a high number of dengue incidence. Most reported cases are observed mainly in the populated cities of Colombo, Gampaha and Kalutara indicating that crowded cities are more likely to be affected due to this. Colombo specifically has been the main city where the disease has been affecting the greatest number of individuals over the past five years with nearly ten to fifteen thousand being affected in 2014, 2015, 2016 and 2018. We can observe a trend in the reported dengue cases being constant over the years with a sudden surge in 2017, in order to reduce the infection better strategies and awareness needs to be created to improve the quality of life index.