Author(s): João Lopes
Introduction: Voice is a determining factor for transgender women to be able to communicate and be recognized by the other as belonging to the desired gender. In voice clinic, exercises of semi-occluded vocal tract and technological resources that act in an adjunct manner are used, aiming to promote better phonatory adjustments, raising the fundamental frequency and vocal tract adjustments such as resonance, intensity, articulation, speed, among others. The work of the speech therapist requires an expanded vision, seeking the integration between voice and body. The present study seeks to understand how the modulation process for acute pitch occurs upon using exercise with a high-strength tube associated with the therapeutic resource of low intensity laser, aiming to evaluate the effectiveness of these two tools when used simultaneously. Material and Methods: The research was based on a case study of a transgender woman. The therapy was based on the application of low intensity laser associated with the use of exercise with high strength tube. The study was approved by the Research Ethics Committee and the participant signed the Informed Consent Form. Anamnesis, application of the Transsexual Voice Questionnaire (TVQ) and evaluation before and after the application of the techniques were performed, through acoustic analysis of the vocal signal and auditory-perceptive evaluation, through the Vocal Profile Analysis (VPA) Protocol. Results and Discussion: There was an increase in variability in the categories of pitch and loudness, absence of crackling and improvement in energy distribution after therapy. The patient used greater voice breathing and there was a predominance in the distribution of articulatory adjustments. Conclusion: Speech therapy promoted an election of the vocal pitch, modified the characteristics of vocal quality and dynamics and generated a sound fluency for the female. It was possible to observe that the greatest change occurred in an auditory way, interfering in the acoustic impression that the other has in relation to this voice, that is, the greatest gain was in the sound filter.
The human being socially categorizes gender as man and/
or woman. Culturally, we are differentiated in feminine and
masculine aspects, which is the role of gender. These rules are
implicitly inserted in our environment through image, behavior
and voice [1].
Those who do not fit need to adjust to feel accepted, as is the case
of the transgender public, who do not identify with the biological
sex. Some people are born with the male sex, although recognize
themselves in the female gender, which constitutes the transgender
woman [2].
Voice is a determining factor capable of identifying the gender
of the speaker. The female fundamental frequency is around 145-
275 Hz and the male frequency is between 80-165 Hz. For a male
voice to be recognized as female, there must be an elevation above
150-160 Hz [3].
Speech also plays an important role, because it allows us to transmit
traits of our personality, psychological and emotional aspects. It has variations that differ from the male voice to the female voice,
such as: speech speed, intonation, intensity, pitch, among other
suprasegmental factors. Therefore, a voice that resembles one’s
new gender identity brings positive aspects, improving the self-
perceived quality of life. While an incoherent voice can generate
a feeling of inadequacy, causing a negative reaction [2].
Approximately 46% of transgender women seek voice feminization
service, because even if they use hormone therapy, no hormone
alone is capable of raising the fundamental frequency, reducing
vocal fold mass or has a lasting effect on pitch [4,2].
Speech-language pathology treatment in vocal confirmation
requires an expanded view, seeking a support between gender
identity and its representation in the female role through voice,
providing a balance between body and voice [5].
The main objectives of this individualized therapeutic proposal
are: change in vocal adjustment, pitch elevation, intensity and
frequency of formants [6].
It is possible to achieve these changes through technological
resources associated with adequate vocal exercises. In voice clinic,
half-occluded vocal tract exercises (SOVTE) are used, which should be performed with some type of vocal tract occlusion, with
the main objective of promoting the interaction between source
(vocal folds) and filter (resonance), favoring vocal performance
[7].
Low intensity laser (LIL) is also used, which contributes to
increasing cellular resistance and vitality, stimulating the tissues
to a rapid return to their functional normality, providing the patient
with a feeling of relief soon after its application, thus accelerating
his/her rehabilitation [8].
The high-strength tube is a variation of SOVTE, produces an
increase in intraoral pressure, decreases effort in the glottis source,
promoting better vocal performance, elevation of the fundamental
frequency, vocal flexibility and a speech with decreased effort
and greater clarity [9].
The Low Intensity Laser is an alternative and noninvasive
therapeutic resource, and has analgesic, anti-edematous, healing,
biomodulator, muscle injury repairing and peripheral nerve
regenerating effects [1,10,11,12].
It is considered an important alternative in the treatment of
inflammatory processes, accelerating healing, pain reduction,
resulting in increased blood circulation and better muscle
performance [13].
Communication is part of the life of the human being, this language,
whether verbal or nonverbal, allows us to provide the other with
the information of what we want to interact with. Several factors
are taken into consideration during a conversation, especially when
no visual clues are provided. Even if the speaker is a stranger, the
listener can have evidence concerning the gender. The way this
voice is perceived helps in the transition process of transgender
women and improves their self-perceived quality of life [2].
Biological factors, social pressure, the media and cultural patterns
are components that induce the vocal image of people [1].
Being recognized by the other as belonging to the gender that is
desired, through a conversation, a call or job interview, is another
obstacle that transgender women need to overcome [4].
The role of the speech therapist goes beyond vocal work, also
worrying about speech, the choice of words, posture, respiratory
pattern, facial expression, gaze, gestures, all these aspects are
important forms of communication [14].
This effort is justified since no studies were found associating the
resource of low-intensity laser with exercise with high-strength
tube, making it necessary to understand how the modulation
process for acute pitch occurs in transgender women, upon using
these two techniques concomitantly.
In view of the above, the objective of the research is to evaluate
the effectiveness of exercise with a high-strength tube correlated
with the therapeutic resource of low-intensity laser in modifying
the vocal quality of a transgender woman.
This research is a case study of a transgender woman, whose participation was approved by the Human Research Ethics Committee, under the number: 2.376.533. The participant received clarification and agreed to participate voluntarily, signing the Informed Consent Form.
The sound was recording, with the emission of the months of the
year and chained speech, with a digital recorder (Sony, Model
ICD-PX470), positioned 10 cm away towards the patient’s mouth,
the stored signal had its initial and final parts cut, the analyses
were made before the techniques and after eight sections, being
performed once a week. The recordings were submitted to vocal
acoustic analysis in voxmetria 2.7 (CTS Informática) and auditory-
perceptive analysis, through the Vocal Profile Analysis (VPA)
Protocol, by John Laver (1980), translated and adapted for the
Brazilian Portuguese by Camargo and Madureira (2008). The
VPA was conducted by two voice expert judges.
Specific exercises were worked for pitch elevation and fundamental
frequency of the patient exclusively part of this research.
The participant received a rigid plastic straw of 8.7 cm in length
and 1.5 mm in diameter, being instructed to keep it between the
lips, slightly occluded and vocalize the sound of the vowel [U], in
high frequency and comfortable intensity. After the demonstration
of the exercise, the participant was asked to perform the sound for
three minutes, breathing when necessary, and, simultaneously, the
laser was applied with the time of four joules, infrared wavelength,
in four points of the larynx: higher region of the thyroid cartilage,
cricothyroid space and in the cricothyroid muscle.
D.F., 20 years old, student, sought the aforementioned outpatient
clinic with the following complaint: “my voice does not suit me”
(SIC). According to the patient, her voice is too deep, which makes
her feel embarrassed when she needs to speak in public. “I avoid
communicating more and more every day, because I do not feel
comfortable when I have to express myself” (SIC). Regarding
vocal health, D.F. denies the use of cigarettes and alcoholic
beverages. Her last videolaryngostrostroboscopy examination
revealed that she had no laryngeal alterations, especially related
to vocal folds. The patient reports that, when she speaks on the
phone, people get confused about how to treat her, even when she
says her social name. Her expectation is “to have a higher-pitched
voice that matches her physical appearance” (SIC).
In the anamnesis, the Transsexual Voice Questionnaire (TVQ)
(APPENDIX A) was used to collect data regarding her daily vocal
activities, medication use, pre-existing diseases and expectations
regarding treatment. In TVQ, the patient reported undergoing
hormone treatment with the Perlutan injectable drug once a month.
In the speech-language evaluation, upper, mixed breathing,
pneumophonoarticulatory incoordination, medium to deep pitch,
adequate loudness, laryngopharyngeal resonance, median to slow
speech speed, precise articulation and vocal quality with a slight
pitch drop to deep were observed.
The patient was worked on vocal orientation and awareness,
elevation of the fundamental frequency, phonation in smile and
articulatory sharpness, exploration of different emissions and
ascending modulation at the end of emissions, modification of the
parameters of intonation, resonance, vocabulary, pronunciation,
articulation and physiognomic and gestural expressiveness during
speech.
The Vocal Profile Analysis (VPA) Protocol aims to describe the
most striking characteristics in vocal quality and vocal dynamics
aspects, under the phonetic theory perspective [15].
The results of the auditory-perceptive evaluation occurred in two moments: before and after therapy.
What stands out is the prosodic aspects evaluated in the pre-therapy, namely: grade 1 refers to a small difference in relation to the
neutral adjustment, grade 2 - slight difference in relation to the neutral adjustment and grade 3 - moderate difference in relation to
the neutral adjustment [16].
In the pre-therapeutic moment, the patient presented little pitch variability with moderate grade, mild grade for high average setting,
wide extension for both pitch and loudness and little loudness variability. The other settings are slight in relation to the neutral setting.
The presence of high-grade tension was observed compared with relaxation.
In the post-therapeutic period, the crackling voice is no longer perceived. As for the prosodic traits, there were moderate settings in
high pitch average, wide pitch and loudness extension and an improvement in variability.
There was a decrease in tension, the patient presented a more relaxed voice, in addition to a better division in the articulatory features.
Chart 1: Auditory-perceptive analysis of vocal dynamics - Before and After Treatment, respectively:
| II- PROSODIC TRAITS | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| CATEGORY | FIRST ANALYSIS | SECOND ANALYSIS | ||||||||
| NEUTRAL | NON-NEUTRAL | SETTING | NORMAL | ABNORMAL | ||||||
| Normal | Abnormal | 1 | 2 | 3 | 1 | 2 | 3 | |||
| 1. PITCH | X | X | High Average | X | ||||||
| Low Average | X | |||||||||
| Wide Extension | X | |||||||||
| Reduced Extension | X | |||||||||
| Great Variability | X | |||||||||
| Low Variability | X | |||||||||
| 2.CONSISTENCY | Tremor | |||||||||
| High Average | X | |||||||||
| 3. LOUDNESS | Low Average | X | ||||||||
| Wide Extension | X | |||||||||
| Reduced Extension | X | |||||||||
| Great Variability | X | |||||||||
| Low Variability | X | |||||||||
| II- PROSODIC TRAITS | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| CATEGORY | FIRST ANALYSIS | SECOND ANALYSIS | ||||||||
| NEUTRAL | NON-NEUTRAL | SETTING | NORMAL | ABNORMAL | ||||||
| Normal | Abnormal | 1 | 2 | 3 | 1 | 2 | 3 | |||
| 1. PITCH | X | X | High Average | X | ||||||
| Low Average | X | |||||||||
| Wide Extension | X | |||||||||
| Reduced Extension | X | |||||||||
| Great Variability | X | |||||||||
| Low Variability | X | |||||||||
| 2.CONSISTENCY | Tremor | |||||||||
| High Average | X | |||||||||
| 3. LOUDNESS | Low Average | X | ||||||||
| Wide Extension | X | |||||||||
| Reduced Extension | X | |||||||||
| Great Variability | X | |||||||||
| Low Variability | X | |||||||||
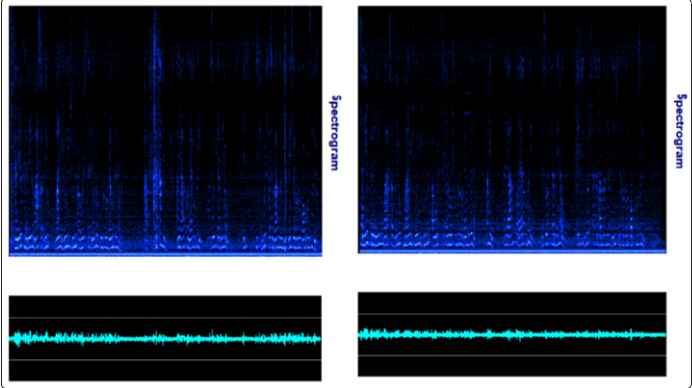
Figure 2: Visualization of spectrographic records in the Pre and Post therapy moments, respectively:
We have the spectrographic layout. What stands out is the amount of acoustic turbulence in the first figure, this term is linked to the
accumulation of secretion, the harmonics become tangled and the predominance of basal frequencies [17].
There are differences, although small, between one tracing and another. In the second file, there is a better balance of sound energies.
Possibly there was an adjustment and the recruitment of the thyroetenoid (TE) muscle decreased, with a participation of the cricothyroid
(CT) muscle more present.
| STATISTICS (from 0.00s to 24.12 s) |
|
|---|---|
| Mode F0: 212.96 Hz | |
| Mean F0: 217.22 Hz | Mean Intensity: 60.89 dB |
| Minimum F0: 161.87 Hz | Minimal Intensity: 55.05 dB |
| Maximum F0: 364.55 Hz | Maximal Intensity: 71.08 dB |
| Stand. Deviation F0: 28.22 Hz | Stand. Dev. Intensity: 3.92 dB |
| Time with Voice Percentage: | 47.05% |
| Voiceless Time Percentage: | 52.95% |
| Sound Time Percentage: | 100.00% |
| Silence Time Percentage: | 0.00% |
| F0 Variability: 202.68 Hz 14 semitones |
| STATISTICS (from 0.00s to 24.12 s) |
|
|---|---|
| Mode F0: 209.49 Hz | |
| Mean F0: 215.37 Hz | Mean Intensity: 59.58 dB |
| Minimum F0: 165.61 Hz | Minimal Intensity: 55.27 dB |
| Maximum F0: 382.92 Hz | Maximal Intensity: 68.64 dB |
| Stand. Deviation F0: 28.41 Hz | Stand. Dev. Intensity: 3.09 dB |
| Time with Voice Percentage: | 47.05% |
| Voiceless Time Percentage: | 52.95% |
| Sound Time Percentage: | 100.00% |
| Silence Time Percentage: | 0.00% |
| F0 Variability: 217.31 Hz 15 semitones |
Figure 3: Visualization of numbers in the pre and post treatment files, respectively
The graphs demonstrate the main statistics of the voice. What
drew our attention is the amount of semitones. states that a full
voice requires 20 semitones in chained speech [17].
We have a slight increase in semitones in Figure 2, although it
remains below the literature. At the same time, the f0 difference
increased, the fundamental frequency variability improved and the
intensity decreased. What can be seen is that there was a change,
although discrete, between the first and second samplings. Possibly
the person promoted less effort and obtained better vocal fluidity.
The scope of this work reflects an analysis of the variation of
vocal quality of a transgender woman at two distinct moments. We
sought to analyze, through the auditory-perceptive and acoustic
evaluation, the competence of exercise with high-strength tube
associated with the therapeutic resource of low intensity laser in
the elevation of the vocal pitch.
There was an improvement in variability in the pitch and loudness
categories, absence of crackling after therapy. The patient used more
thee breathing and there was a predominance in the distribution
of articulatory adjustments, where the articulation of vowels was
worked with the purpose of increasing the mandible opening so
that the voice gained higher harmonics in the middle of the words,
which provides a higher pitch to the voice, accentuation of the
phonemes in a melodic way and increase at the end of the sentences
to maintain the high pitch, always seeking the most feminine
pattern, which is also possible to visualize in the spectrographic
analysis (Figure 2) and in the comparison of statistical analysis
(Figure 3f), complementing the result found in the auditory-
perceptive analysis. The correlation between auditory and acoustic
data is the basis of clinical, diagnostic and therapeutic reasoning
of the speech therapist [17].
Language studies aimed at prosodia allow understanding new
social and individual dimensions, through the application of
various methods to investigate the auditory-perceptive aspects
that help understand the adjustments of the vocal and phonatory
tract of a subject during communication [16].
What makes the patient seek the treatment of vocal confirmation
is the way the other perceives his/her voice, that is, the perceptive
nature of vocal quality. Observing these resources used in the
settings of this speaker, it is also noticed that, with this change
in the voice quality and dynamics, there is a new construction of
identity, whose supraglottis vocal setting was worked, promoting
a new standard of vocal quality for this subject [1].
Thus, to raise the fundamental frequency, it is necessary to make
the vocal folds vibrate more times per second. Thinking about the
biomodulatory effect provided by low intensity laser, this effect
causes a movement of muscle fibers and the associated use of the
rigid tube increases vocal flexibility, activating and lengthening
the cricothyroid muscle, which is responsible for producing the
high pitch, providing a sensation of vocal fullness [1,17].
Exercise with a high-strength tube has shown positive results in the
short term, both for vocal improvement and in the treatment and
prevention of dysphonia. It is understood that partial occlusion of
the lips leads to an increased impedance of airflow in the anterior
part of the oral cavity, resulting in a sensation of vibration in the
filter (resonance) and an increased intraoral pressure, being the air
stream directed to the straw, thus being performed as a sound [18].
The human being has unique characteristics that contribute to
vocal production. The voice is an individual marker and should be
worked in a way that offers the patient comfort with the expression
of gender in social interactions. When a characteristic is not in
conformity with the desired gender, it can alter self-esteem,
impacting social relationships and impairing their confidence to
communicate, generating feelings of inadequacy and frustration
[19].
Transgender people are not yet fully recognized by the state,
often finding barriers that prevent them from competing in the
labor market. One of the reasons that hinder their insertion is still
discrimination at work and the different name in the identification
document. This observation seems to justify some findings, if this
subject makes use of his/her social name and has a voice and body
that are in accordance with the desired gender, certain questions
would be smaller or even not present [20].
Promoting the social inclusion of this population and inserting
them in the labor market is part of the humanized treatment that
we perform with this audience [4,21,22].
The speech therapy performed with the association of low intensity laser with exercise with high-strength tube promoted an increase of the vocal pitch, modifying the characteristics of vocal quality and dynamics, generating a sound fluency for the female. It was possible to observe that the greatest change occurred in a perceptual auditory way, interfering in the acoustic impression that the other has in relation to this voice, that is, the greatest gain was in the sound filter.
1. LOPES J, DORFMAN, MEKY DORNELAS RA (2019)
voice of the transgender person - challenges and possibilities
in the vocal clinic. In: LOPES, L .; MORETI, F .; RIBEIRO,
L. L .; PEREIRA, E. C. Fundamentals and Current Events
in Clinical Voice. 1st ed. Rio de Janeiro: Thieme Revinter
Publications p-173-178.
2. SCHMIDT JG (2018) Voice challenge in transgender women:
trans women self-perception of voice handicap as compared
to gender perception of naïve listeners. Revista CEFAC, São
Paulo 20: 79-86.
3. SANDOVAL Z MS (2019). Immediate effect of semi-
occluded vocal tract therapy on acoustic parameters in
transsexual people between 13 and 24 years of age. Journal
of Research in Speech Therapy,Chile 9: 67-79.
4. HANCOCK A, HASKIN G (2015) Speech-Language
Pathologists’ Knowledge and Attitudes Regarding Lesbian,
Gay, Bisexual, Transgender, and Queer (LGBTQ) Populations.
American Journal of Speech-Language Pathology, Washington
24: 206-221.
5. SILVA TR, SILVEIRA MCC (2019) The speech therapist’s
look at the body and the voice in transsexuality. IV International
Seminar UNDERSTANDING GENDER - student body,
resistant body: from chaos to mud, Pernambuco v-1.
6. GÓMEZ-RAYA A (2018) Speech therapy intervention in
the feminization of the voice in transsexuals: bibliographic
review. Journal of Research in Speech Therapy 8: 21-42.
7. CIELO CA (2013) Semi-occluded vocal tract exercises:
literature review. CEFAC Magazine, São Paulo 15: 1679-
1689.
8. CATãO MHCV (2013) Evaluation of the effectiveness of low-level laser in the treatment of temporomandibular
disorders: randomized clinical study. CEFAC Magazine, São
Paulo 15: 1601-1608.
9.COSTA CB (2011) Immediate effects of the phonation into
a straw exercise. Brazilian Journal of Otorhinolaryngology,
São Paulo 77: 461-465.
10.ASSIS TO, SOARES MS, VICTOR MM(2012) The use of
laser in the rehabilitation of temporomandibular disorders.
Physiotherapy in Motion, Paraná 25: 453-459.
11.GOMES CF, SCHAPOCHNIK A (2017) The therapeutic
use of the Low Intensity LASER (LBI) in some pathologies
and its relationship with the performance in Speech Therapy.
Communication Disorders, São Paulo, 29: 570.
12.MATOS AS (2018) Laser therapy applied to orofacial
motricity: perception of members of the Brazilian Orofacial
Motricity Association - Abramo. Revista CEFAC, São Paulo
20: 61-68.
13.ALVES VMN, FURLAN RMMM, MOTTA AR (2019)
Immediate effects of photobiomodulation with low-level
laser therapy on muscle performance: an integrative literature
review. Revista CEFAC, São Paulo v-21.
14.SEGER MF (2018) V oz in transit: gender and speech therapy
in the “vocal readjustment” of trans people. 2018. 107 f.
Dissertation (Master in Public Health) - Institute of Social
Medicine, State University of Rio de Janeiro, Rio de Janeiro
p-50-52
15.SILVA MFBL (2017) Vocal quality assessment: methodological approach for a perceptive data analysis.
Revista CEFAC, São Paulo 19: 831-841.
16.CAMARGO ZA, MADUREIR AS (2008) Vocal assessment
from a phonetic perspective: preliminary investigation.
Communication Disorders, São Paulo 20: 77-96.
17.BEHLAU MMADAZIO, GFEIJÓ DPONTESP,(2008) Voice
assessment. In: BEHLAU, M. (org). VOICE, The Expert’s
Book. São Paulo Revinter 1: 85-132.
18.PAES SM, BEHLAU M (2017) Dosage dependent effect
of high-resistance straw exercise in dysphonic and non-
dysphonic women. CoDAS, São Paulo 29: e20160048.
19.CROW KM, VANMERSBERGEN MPAYNE AE (2019)
Vocal Congruence: The Voice and the Self Measured by
Interoceptive Awareness. Journal of Voice, Tennessee P-1-14.
20.SILVA ACM, OLIVEIRA JV, FERREIR AP (2019) Sis (cis)
theme of the labor market and the exclusion of transsexuals.
In: ORLANDINI, M. L. S. R .; PALUMA, T .; SOUZA, A.
M. A. (org). Challenges of contemporary work. Uberlândia:
EDUFU p-42-44.
21.LOPES JC (2019) Case report of speech language therapy
work for voice adequacy of a male transgender. Clinical
Practice, Brasil 16: 1293-1300.
22.MEDINA V, SIMÕES-ZENARI M, NEMR NK (2015)
Acoustic vocal analysis: effect of auditory-visual training
for Speech Therapy students. Audiology - Communication
Research, São Paulo 20: 123-129.